Download
1 / 14
150 likes | 405 Views
Euthanasia and Assisted Suicide: Acts of mercy. By: Mackenzie race. What is euthanasia and assisted suicide?. Euthanasia is the administration of lethal medicine to a patient in order to end life.

E N D
Euthanasia and Assisted Suicide: Acts of mercy By: Mackenzie race
What is euthanasia and assisted suicide? • Euthanasia is the administration of lethal medicine to a patient in order to end life. • Assisted suicide is legally receiving assistance from a physician in care to end life – there are four different types of assisted suicide Euthanasia and assisted suicide is legal in one state, Oregon. In 1994 the Death with Dignity act was passed legalizing assisted suicide to those who meet the qualifications.
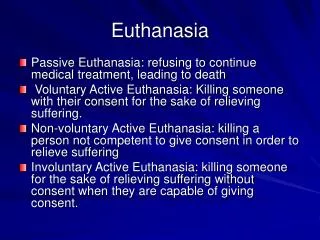
The four types of assisted suicide • Active Voluntary • Directly causing death (mercy killing) with the consent of the patient • Active Involuntary • Directly causing death (mercy killing) without the consent of the patient • Passive Voluntary • Withholding or withdrawing life-sustaining measures with the consent of the patient • Passive Involuntary • Withholding or withdrawing life-sustaining measures without the consent of the patient.
The primary focus and thesis • Physician Assisted suicide should be legalized WHY? • Preserves dignity of the patient – in both the manner they wish to die and the manner they wish to be remembered among relatives • Provides the patient with another option, although euthanasia is not a treatment it is an alternative to suffering through the last months of life • It is a merciful and humane act that follows strict legal protocol (if legalized in all states) • The patient is protected from malevolent intentions of the physician and is always able to back out of euthanasia if the lethal medicine has not yet been administered.
Killing and let die • Killing – killing occurs when a physician directly causes the death of the patient with consent of the patient • Letting die – occurs when a physician and patient agree not to take life-sustaining measures (i.e. removing a patient from a respirator, not preforming a vital surgery, not administering antibiotics or medicines). The difference between these two terms is that killing is seen as socially unacceptable, while letting a patient die is seen as a physician in care dutifully respecting the patient’s wishes. Killing is the direct cause of the death, while letting die is letting the underlying disease kill
In the first case, Smith stands to gain a large inheritance if anything should happen to his six-year-old cousin. One evening while the child is taking his bath, Smith sneaks into the bathroom, drowns the child, and arranges things so that it will look like an accident. In the second case, Jones also stands to gain if anything should happen to his six-year-old cousin. Like Smith, Jones sneaks in, planning to drown the child in his bath. However, as he enters the bathroom Jones sees the child slip, hit his head and fall face down into the water. Jones is delighted; he stands by, ready to push the child’s head back under if necessary, but it is not necessary. With only a little thrashing about, the child drowns all by himself, “accidently,” as Jones watches and does nothing. Smith killed the child, while Jones merely let the child die. That is the only difference between the two cases. Did either man behave better than the other, from a moral point of view?
Why the argument becomes invalid • Mercy killing and letting a patient die are essential the same thing • The general belief is that killing a person is morally worse than letting a person die • The claim that physician assisted suicide is murder prevents legislation from passing, although there is no moral difference between the two • Either way, the physician must play an active and casual role in the death of the patient – the only difference between the cases we just read is that a physician does so with good intentions.
Autonomy argument • Every individual has autonomy - or self-governance – to act upon things they believe will fulfil their vision of life • Each patient should have the opportunity to weight the benefits and burdens of euthanasia – legally. • The patient’s rights to make their own fully competent decision of whether or not life is worth living should be respected both constitutionally and morally. • There should be no punishment for a physician respecting the wishes of the patient, it is the patient’s own personal decision to their own personal deaths – as they see how their lives should be fulfilled.
“People have an interest in making important decisions about their lives in accordance with their own conception of how they want their lives to go. In exercising autonomy or self-determination, people take responsibility for their lives; since dying is a part of life, choices about the manner of their dying and the timing of their death are, for many people, part of what is involved in taking responsibility for their lives. Many people are concerned about what the last phase of their lives will be life, not merely because of fears that their dying might involve them in great suffering, but also because the desire to retain dignity and as much control over their lives as possible during this phase... There is no single, objectively correct answer as to when, if at all, life becomes an burden and unwanted. But that simply points up the importance of individuals being able to decide autonomously for themselves whether their own lives retain sufficient quality and dignity to make life worth living.” Robert Young, “Voluntary Euthanasia,” The Stanford Encyclopedia of Philiosophy(winter 2007), ed. Edward N. Zalta
Slippery slope theory • The general public fear that if active voluntary euthanasia is legalized, the strict protocol will be breached by physicians across the country • The belief that the legalization of one type of euthanasia will lead to the other types of euthanasia without patient permission will become condoned. • Physicians will urge debilitated, mentally ill, or uninsured patients towards assisted suicide • Physicians will start pushing unsure patients towards suicide
Why the theory is unjust • There is extremely strict legal protocol in administering lethal doses of medicine or preforming euthanasia. • Any breech of protocol will result in the treatment of the offender as a murder – no consent of the patient qualifies the death as manslaughter in the courts. • Patients should be comforted with the option of death instead of being forced to suffer through painful illnesses or vegetative states that could last for decades without relief. • Physicians will not administer a lethal injection for what is believed to be a regular check-up shot – the job of a physician is to care for patients as best they can and to respect their wishes. • The theory is irrational – doctor-patient relationships are strictly to ensure the health of the patient, lethal medicine is only administered upon request. • For the theory to work there must be good evidence of the consequences – since euthanasia is legal in one state there is no evidence of abuse thus far.
How to qualify for the right to death (for residents of Oregon) • Must be 18 years of age or older • Must be a legal resident of Oregon • Must have a terminal illness that will cause death within 6 months • Lethal medicine must be requested twice orally (on separate occasions) – and a written request signed by the patient once before the physician may respect the right to death • The physician must inform the patient of ALL other available treatments before prescribing the medicine • The doctor can deny a right to death if the patient is believed to be depressed and order therapy treatments instead of lethal medicine.
conclusion • The legalization of euthanasia and assisted suicide would prevent the suffering and trauma of patients through the last stages of their life • Constitutionally the right to autonomy is respected elsewhere; it should be respected medically as well. • There is no moral difference between mercy killing and letting die of the physician – a doctor does either with good intentions, and is losing life whether directly causing the death or not. • There is no statistical proof of abuse of euthanasia – therefore the slippery slope theory does not exist. The only way to determine bad consequences of euthanasia is by evidence that the legalization will lead to probable and serious abuse of the right by physicians.
References • Bellenir, K. E. (2005). Section 10.1. In Mental health disorders: Health reference series. Detroit: Omnigraphics. • Coombs, B. L. (2005, June 5). Staff. End of Life Planning and Palliative Care. Retrieved February 22, 2014, from https://www.compassionandchoices.org/who-we-are/compassion-choices-staff/ • Telfer, S. (2012, December 18). Staff. Death with Dignity National Center. Retrieved February 22, 2014, from http://www.deathwithdignity.org/aboutus • Vaughn, L. (2013). Euthanasia. In Contemporary moral arguments: Readings in ethical issues (2nd ed.). New York: Oxford University Press. • Smith, E. (2014, October 24). Euthanasia Prevention Coalition. Euthanasia Prevention Coalition. Retrieved March 3, 2014, from http://www.epcc.ca/