Download
1 / 15
170 likes | 450 Views
Neisseria meningitidis Case Study. Dr. Jennifer Coetzee. Clinical Scenario. 19 year old engineering student Presents to campus health in morning, c/o flu-like symptoms, feeling unwell Sent home with paracetamol, vitamin C

E N D
Neisseria meningitidis Case Study Dr. Jennifer Coetzee
Clinical Scenario • 19 year old engineering student • Presents to campus health in morning, c/o flu-like symptoms, feeling unwell • Sent home with paracetamol, vitamin C • Late afternoon found by roommate, delirious, feverish, severe headache, rash • Diagnosed at E.R. with suspected meningitis • Lab confirms diagnosis of meningococcal meningitis, septicemia
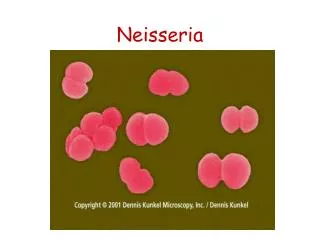
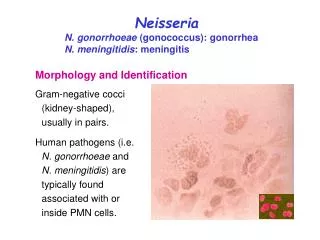
Microbiological Characteristics • Gram negative diplococci • Grows on chocolate agar • Oxidase positive, ferments glucose, maltose • Immunologic reactivity of capsular polysaccharides basis for serogrouping • At least 13 serogroups • A, B and C cause most cases of disease worldwide
Neisseria meningitidis (Arrow) in Cerebrospinal Fluid (Gram's stain, x1000) Rosenstein N et al. N Engl J Med 2001;344:1378-1388
Cross-Sectional View of the Meningococcal Cell Membrane Rosenstein N et al. N Engl J Med 2001;344:1378-1388
Conditions for Invasive Disease • 4 conditions to be met for invasive disease to occur: • Exposure to a pathogenic strain • Colonisation of nasopharyngeal mucosa • Passage through that mucosa • Survival of the meningococcus in the bloodstream
Colonization of Neisseria meningitidis in the Nasopharynx and Entry into the Bloodstream and Cerebrospinal Fluid Rosenstein N et al. N Engl J Med 2001;344:1378-1388
Pathogenesis • Humans only natural reservoir • Transmitted from nasopharynx by aerosol/ secretions • 10% of population colonised at any time • Attaches via pili to nonciliated columnar epithelial cells • Small percentage will penetrate mucosa, enter blood stream, and cause disease • Carriage results in protective antibodies
Virulence Factors • Polysaccharide capsule • Protects against complement mediated lysis • Anti-phagocytic • Capsule switching • Endotoxin • Lipo-oligosaccharide • Releases outer-membrane vesicles with endotoxin, outer membrane proteins, phospholipids, capsular polysaccharides • IgA protease • Promotes attachment to mucosal surfaces
Pathogenesis • Upon invasion of blood stream, activation of 3 main pathways: • Complement system • Regulates degree of hypotension • Patients with complement deficiency have increased susceptibility to meningococcal disease, but disease is less severe • Inflammatory response • Coagulation and fibrinolytic pathway
Risk Factors • 6 – 24 month old babies most susceptible • Role of maternal antibodies • Terminal complement deficiency – up to 6000x higher risk, also recurrent disease • Functional / anatomical asplenia • Household crowding, urban residence • Active or passive tobacco smoke • Concurrent viral infections of the upper respiratory tract
Management • Diagnosis! • Cerebrospinal fluid or blood cultures • Culture or antigen detection • Antibiotics ASAP • Supportive measures
Prevention • Notify Department of Health • Chemoprophylaxis to all household contacts • Also close contacts • ? Healthcare personnel • Chemoprophylactic regimens (for reference only): • Rifampicin 600 mg po BD x 4 doses • Ciprofloxacin 500 mg po stat • Ceftriaxone 250 mg po stat
Vaccines • Quadrivalent polysaccharide vaccine against serogroups A, C, Y and W-135 available • Antibody responses are serogroup-specific and independent • Recommended for healthcare workers, also tertiary students • Recommended for the control of outbreaks due to serogroup C • Beware of capsular switch
References • Rosenstein N.E., Perkins B., et al. Meningococcal Disease. N Eng J Med 200; 344:1378-1388 • Emonts M., Hazelzet J.A., et al. Host genetic determinants of Neisseria meningitidis infections. Lancet Infect Dis. 2003; 3:565-575.