Download
1 / 19
190 likes | 329 Views
S I C HEART Study. MELGAR O. MATULAC MD., LEORA FLOR MACAPUGAY MD., MICHAEL REYES MD., KRISTINE TUMABIENE MD., ALRIC MONDRAGON MD . SECTION OF CARDIOLOGY DEPARTMENT OF MEDICINE UNIVERSITY OF THE PHILIPPINES – PHILIPPINE GENERAL HOSPITAL.

E N D
SICHEART Study MELGAR O. MATULAC MD., LEORA FLOR MACAPUGAY MD., MICHAEL REYES MD., KRISTINE TUMABIENE MD., ALRIC MONDRAGON MD .SECTION OF CARDIOLOGYDEPARTMENT OF MEDICINEUNIVERSITY OF THE PHILIPPINES – PHILIPPINE GENERAL HOSPITAL SildenafilImproves Exercise Capacity in Heart Failure:A Meta-analysis
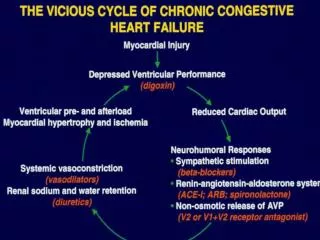
HEART FAILURE OUR CHALLENGE! DISCOVER NEW FORMS OF INTERVENTION TO IMPROVE OVERALL CARDIAC PERFORMANCE FACTS: - 1 in 3 develop HF at age >551 - only 35% surviving 5 years after the first diagnosis.1,2 As HEART FAILURE progresses: PULMONARY HYPERTENSION RV DYSFUNCTION 68 – 78 % (w/ LV dysfunction) MORTALITY 2X Despite advancement in Treatment: - Most HF patients are limited by their EXERCISE AND FUNCTIONAL CAPACITIES affecting their QUALITY OF LIFE Gyse`le S. BleuminkQuantifying the heart failure epidemic:prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. European Heart Journal (2004) 25, 1614–1619 John J McMurrayHEART FAILURE Epidemiology, aetiology, and prognosis of heart failure. Heart 2000;83:596–602 Behling A, Rohde L, Colombo F, et al. Effects of 5’ -Phosphodiesterase Four-Week Long Inhibition With Sildenafil in Patients With Chronic Heart Failure: A Double-Blind, Placebo-Controlled Clinical Trial. Journal of Cardiac Failure. 2008. 14(3):189-97
Endothelial dysfunction in association with heart failure and muscular dysfunction CHF HALLMARK INCREASE IMPEDANCE TO THE RIGHT AND LEFT VENTRICULAR EJECTION DUE TO INCREASE IN PULMONARY AND SYSTEMIC VASCULAR RESISTANCE THERAPEUTIC GOAL IN CHF IMPROVE THE OVERALL CARDIAC PERFORMANCE IS REDUCTION IN PULMONARY VASCULAR RESISTANCE ENDOTHELIAL DYSFUNCTION www.sciencedirect.com Zhi You Fang.Mechanisms of exercise training in patients with heartfailure. AHJ 2002
SILDENAFIL(PHOSPHODIESTERASE 5 INHIBITOR) Sildenafil citrate - selective PDE5 inhibitor, acts on NO/cGMP pathway - First synthesized in 1989, ANGINA as the particular indication. - 1991 – Clinical development indicated for Angina, similar to nitrates but w/o tachyphylaxis. - Penile erection as commonly reported side effect. ovebucketblog.com Parnham. Milestone in Drug Therapy. Library of Congress 2004
RESEARCH QUESTION Among patients with chronic heart failure and secondary pulmonary hypertension, will long-term treatment with PHOSPHODIESTERASE – 5 INHIBITOR (Sildenafil) improve exercise capacity?
METHODOLOGY LITERATURE SEARCH Search Strategy: Medline, Embase, Cochrane Library Search Terms: Sildenafil, Phosphodiesterase-5 inhibitor, Heart Failure Limited to: Humans subjects & RCT’s Secondary Search: Bibliographies of RCTs RESEARCH QUESTION • ELIGIBILITY CRITERIA: • - RCTs: Stable Heart Failure on • standard HF Therapyrandomized • to either placebo or Sildenafil • Chronic LV systolic dysfunction • (EF <40% who underwent • cardiopulmonary testing before • and after Sildenafil treatment 49 citations Excluded: 24 studies 25 articles evaluated • Studies EXCLUDED: 17 • 6 RCTs: Acute use • 2 RCTs: IV Sildenafil • 1 RCT : Preserved EF • 3 Trials: Cardiac Transplant • 2 RCTs: (+) Lung Problem • 4 RCTs: (+) other drugs • 3 RCTs: Erectile Dysfunction 4 RCTS satisfied the eligibility criteria Data extraction,Qualityassesment & Synthesis of evidence
OUTCOMES MEASURED • PEAK VO2 • - measure of O2 consumption during peak exercise • most widely used parameter to predict survival, re-hospitalization • and risk stratification in patients with CHF1 • Low peak VO2 < 12.2ml/kg/min: 66% 1 yr cardiac mortality • VE/VCO2 Ratio ( Ventilation/ CO2 production ratio)2 • Excessive ventilatory response to exercise perceived as breathlessness • Measure of ventilatory efficiency: Increase ventilation – premature • exhaustion of ventilatory reserve • Risk predictor in patients w/ CHF: Higher VE/VCO2 – higher mortality1 • PRIMARY OUTCOMES: • CHANGES IN EXERCISE CAPACITY • VO2 at Peak exercise • VE/VCO2 Slope • SECONDARY OUTCOMES: • Pulmonary artery pressures • Left ventricular ejection fraction • SAFETY OUTCOMES: • Headache • Flushing
SC: Single center, RCT: Randomized controlled trials, DB: Double blind, FMD: Flow mediated dilatation, QOL: quality of life, SV: Stroke volume, SVR: Systemic vascular resistance, MPAP: Mean pulmonary artery pressure, PWP: Pulmonary wedge pressure, PVR: Pulmonary vascular resistance, LV EF: Left ventricular ejection fraction,
NYHA FC: New York Heart Association Functional Class, FEV: Forced expiratory volume, FVC: Forced vital capacity, LVEF: Left ventricular ejection fraction, DM: Diabetes milletus, PVD: Peripheral vascular disease, AF: atrial fibrillation, HF: Heart Failure, PH: Pulmonary hypertension, AS: aortic stenosis, ED: Erectile dysfunction
RESULTS AND DISCUSSION SildenafilImproves Exercise Capacity in Heart Failure: A Meta-analysis(SIC Heart Study)
Mean Change in Peak VO2 at the END OF STUDY: SIGNIFICANT INCREASE Change in Peak VO2 from baseline
Mean Change in Peak VO2 at 1 – 3 months Mean Change in Peak VO2 at 6 months SIGNIFICANT IMRPOVEMENT in PEAK VO2 at 3rd and 6th month
Mean Change in VE/VCO2 at the END OF STUDY: SIGNIFICANT DECREASE Change in VE/VCO2 from baseline
Mean Change in PAP at the END OF STUDY: SIGNIFICANT DECREASE Change in Pulmonary Artery Pressure from baseline
Mean Change in LVEF at the END OF STUDY Change in LVEF from baseline
Occurrence of HEADACHE during Sildenafil Treatment NO SIGNIFICANT DIFFERENCE in SAFETY OUTCOME WITH PLACEBO Occurrence of FLUSHING during Sildenafil Treatment
CONCLUSION AND RECOMMENDATION • Sildenafil improves exercise capacity as evidenced by improvement in Oxygen uptake, Ventilatory efficiency and Pulmonary pressure reduction without significant adverse effects • FUNCTIONAL CAPACITY • CLINICAL STATUS • QUALITY OF LIFE • SILDENAFIL could be an ADJUNCT to standard medical therapy for chronic heart failure • Warrants LARGER LONG TERM CLINICAL TRIALS SildenafilImproves Exercise Capacity in Heart Failure: A Meta-analysis(SIC Heart Study)
SICHEART Study MELGAR O. MATULAC MD., LEORA FLOR MACAPUGAY MD., MICHAEL REYES MD., KRISTINE TUMABIENE MD., ALRIC MONDRAGON MD .SECTION OF CARDIOLOGYDEPARTMENT OF MEDICINEUNIVERSITY OF THE PHILIPPINES – PHILIPPINE GENERAL HOSPITAL SildenafilImproves Exercise Capacity in Heart Failure:A Meta-analysis