Download
1 / 41
510 likes | 1.03k Views
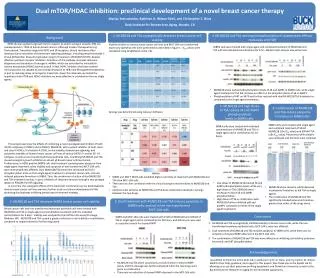
Developing Personalized Therapy Breast Cancer: Gene Expression Signatures. Alex E. Denes , M.D. Lake of the Ozarks September 26, 2010. Outcomes of Adjuvant Chemotherapy in Breast Cancer. Walgren et al. JCO 2005;23:7342-7349. Objectives. Case: Chemotherapy or hormonal therapy

E N D
Developing Personalized Therapy Breast Cancer: Gene Expression Signatures Alex E. Denes , M.D. Lake of the Ozarks September 26, 2010
Outcomes of Adjuvant Chemotherapy in Breast Cancer Walgren et al. JCO 2005;23:7342-7349
Objectives • Case: Chemotherapy or hormonal therapy • Who should receive adjuvant chemotherapy? • The birth of gene-expression signatures: Intrinsic breast cancer subtypes • Gene Expression Signatures under development • 70-gene Signature (MammaPrint) • 21-gene Signature ( Oncotype DX) • Clinical and economic impact of gene expression profiling
Clinical Case 62 y/o WF with newly diagnosed IDC R breast • MMG / Ultrasound 1.2 x 1.2 cm mass at 10 o’clock + surrounding microcalcifications + several suspicious axillary LNs • s/p modified radical mastectomy • Surgical Path – 2.1 cm lesion consisting of IDC mixed with DCIS; intermediate grade; 11 (-) LNs; ER+/PR+/HER-2-; T2N0M0 • What is her risk of recurrence? • What is her risk of death? • What is your recommendation for adjuvant therapy? • Tamoxifen • Aromatase Inhibitor • Hormonal therapy + chemotherapy
Who Should Receive Adjuvant Chemotherapy? • 65% of women with invasive breast cancer have LN(-) disease • Adjuvant chemotherapy improves DFS and OS in pre- and postmenopausal women <70 with LN+/- breast cancer • NSABP B-14 & B-20 showed the benefit of tamoxifen & chemo in ER+/LN- breast cancer • Likelihood of distant metastases at 10 years is about 15% • 85% of pts are over treated if chemo given to all patients • Those with poor prognostic features benefit most from chemotherapy • Main clinical prognostic factors: age, tumor size, axillary LN status, tumor histology, grade, and hormone-receptor status How else can we classify these tumors?
Intrinsic Breast Cancer Subtypes described by Perou et al. Luminal A Luminal B HER2+ Basal-like Express ↑ amounts Of luminal cyto- Keratins & genetic Markers of luminal Epithelial cells of Normal tissue Express ↑ levels of EGFR, c-kit, & growth factors like hepatocyte growth factor and IGF Sotiriou, C. et al. NEJM, 2009.
Gene Expression Profiles or “Signatures” • Composed of a selection of genes felt to provide prognostic or predictive information about tumors • A number of gene expression signatures have been developed to help identify those patients at low or high risk for recurrence • May avoid chemotherapy administration to patients at low risk or patients who will likely not benefit from treatment
Mammaprint: Development of the 70-Gene Signature • DNA microarray analysis of 78 breast primary tumors (untreated) • Pts were <55 years of age with T1-2/N0 disease • Pts selected based on outcome: Distant metastases within 5 years • Statistical analysis, “supervised classification,” identified 231 genes correlated with disease outcome Top 70 genes selected • Genes that regulate cell cycle, invasion, metastasis, & angiogenesis • Patients categorized as “good prognosis” or “poor prognosis.” • Found to be a better predictor of distant metastases within 5 years than all clinical variables in this study • Odds ratio (distant metastases): poor to good prognosis groups = 15 Van ’t Veer, L. Nature, 2002.
Retrospective Validation of the 70-Gene Signature • 295 women ages ≤ 52 with T1-2, LN-/+ breast cancer • 226 ER+ / 69 ER- • chemo 31%; hormonal 7%; both 7% • 61 pts included in the analysis were used to develop 70-gene signature Van de Vijver. NEJM, 2002.
Prognosis Signature Predictive of End Points (10 years) Probability of Remaining Metastasis-free Overall Survival 995% ±2.6% 85 % ±4.3% 555% ±4.4% 51 % ±4.5% Van de Vijver. NEJM, 2002.
Multivariate Analysis Independent predictors of risk of distant metastasis as a 1st event • 70-gene signature • Tumor diameter • Chemotherapy • Lymph node status • Vascular invasion Authors report that gene signature is predictive of distant mets in LN+ pts Multivariate analysis argues that LN status is independent of gene signature as a predictor Van de Vijver. NEJM, 2002.
TRANSBIG Independent Retrospective Validation Study • Retrospective evaluation of 302 pts from several sites in Europe (age<60, T1-2, LN-) previously untreated • Aim: to examine whether the 70-gene signature had prognostic value independent of the best clinical risk classifications (St Gallens, Nottingham Prognostic Index, & adjuvant online) Buyse, M. J of NCI, 2006.
Does 70-gene Signature have Independent Prognostic Value? • Gene signature adds independent prognostic information to that provided by various risk classifications • The signature remained a statistically significant prognostic factor for time to distant metastases & OS even after adjustment for various risk classifications (HR 2.15 & 2.15, respectively) Buyse, M. J of NCI, 2006.
Forrest Plot of HR for Time to Distant Metastases Clinical Sites • Although, average HR of 2.32 is significant…there was wide variation in the HRs among clinical sites. • Therefore model is very sensitive to variation in patient population Buyse, M. J of NCI, 2006.
Conclusions of Validation Studies • Studies were retrospective • Concern for overfitting with supervised analysis of relatively small sample sizes and large numbers of genes • The first validation study contained 61 patients from study on which the classifier was built • Do the claims exceed evidence?
Prospective Validation of Mammaprint: The MINDACT Trial Risk assessed via Clinicopathological Factors (adjuvant) + Mammaprint 6,000 LN (0-3+) patients High risk Chemo + Endocrine Low risk Endocrine Discordant cases: random assignment to follow genomic vs clinicopathologic result Accrual started 2/07, actively enrolling patients, enrollment 1000/yr, analysis in 2019 Cardoso, F. JCO, 2008.
Oncotype Dx: The 21-Gene Assay • Designed to quantify the risk of distant recurrence in patients with LN(-), ER(+) tumors receiving tamoxifen • RT-PCR was used to quantify gene expression from fixed, parafin-embedded tumor tissue • 250 candidate genes selected based on published literature, genomic databases, & experiments based on DNA arrays on fresh-frozen tissue • Analyzed data from 3 independent studies (447 patients) including tamoxifen-only arm of NSABP trial B-20 to test relation b/w 250 genes and recurrence of breast cancer • From these studies, 16 genes (+5 reference genes) were selected that correlated with proliferation and endocrine response
Levels of Gene Expression Determine Recurrence Score 21-gene assay = 16 outcome-related genes + 5 reference genes Higher expression levels of “favorable” genes = ↓ RS Higher expression levels of “unfavorable” genes = ↑ RS Cutoff points chosen based on Results of NSABP trial B-20 A risk score is calculated from 0 -100 Sparano, J & Paik, S. JCO, 2008.
Prospective Validation Study of 21-Gene Assay • Analyzed tumor blocks of 668 patients on NSABP trial B-14 study that were randomized to tamoxifen • RS was significantly correlated with relapse free interval & OS (p<0.001) • Rate of distant recurrence at 10 years: • Low risk – 6.8% • Intermediate risk – 14.3% • High risk – 30.5%(similar risk to LN+ patients) No distant recurrence (low risk) = 93.2% No distant recurrence (high risk) = 69.5% p<0.001 Paik, S. JCO, 2004.
Other End Points Distant Recurrence as a Function of RS Multivariate Cox Analysis RS predicted distant recurrence independent of age & tumor size The likelihood of distant recurrence ↑ continuously as the RS ↑ Paik, S. JCO, 2004.
Does RS Have Prognostic or Predictive Value? • Oncotype was evaluated in both TAM (n=290) & placebo (n=355) arms of the NSABP B-14 trial to determine its prognostic value in an untreated population • Patients with low (p=0.02) and intermediate (p=0.04) RS derived benefit from tamoxifen, whereas those with high RS (p=0.82) did not • Although sample size limited, seems to indicate that ↓ RS predicts greater benefit to TAM • Population-based external validation study of women with ER+/LN- breast cancer in The Northern California Kaiser Permanente tumor registry, age <75, untreated & TAM • RS was associated with risk of breast cancer death in tamoxifen-treated (p=0.003) and untreated patients (p=0.03) • Prognostic in TAM-treated and untreated pts Paik, S. ASCO Abstract, 2005. Habel, L. Breast Cancer Research, 2006.
Does the 21-Gene Assay Predict Response to Chemotherapy? • NSABP B20 trial: 651 ER+/LN- pts randomized to chemo + TAM (n=424) v. TAM alone (n=227) (ALL PATIENTS) • Chemo – CMF or MF • No distant recurrence - 92.2% (chemo + TAM) v. 87.7% (TAM) • No local/distant relapse - 90.1% (chemo + TAM) v. 83.5% (TAM) • Overall Survival – 89.5% (chemo + TAM) v. 86.4% (TAM) • The TAM alone arm was used in the training set in development of the 21-gene assay Paik, S. JCO, 2006.
Kaplan-Meier Plots for Distant Recurrence 92.2% 87.7% All patients Low Risk RS <18 88% 60% Intermediate Risk RS 18-30 High Risk RS ≥ 31 Paik, S. JCO, 2006.
Relative & Absolute Benefit of Chemotherapy as a Function of RS Low RS mean absolute decrease in distant recurrence rate of -1.1% Intermediate RS no substantial benefit, But the uncertainty in the estimate cannot Exclude a clinically important benefit High RS mean absolute decrease in Distant recurrence rate of 27.6% 27.6% Paik, S. JCO, 2006.
How Often Does the Recurrence Score Affect Treatment? • 89 pts; 3 academic, 1 community institution Recommendation No. % CHT CHT 40 45 HT CHT 3 3 CHT HT 20 23 CHT CHT 20 23 HT Either 3 3 CHT Either 2 2 Either Either 1 1 Lo SS, et al. JCO. 2010: 28: 1671
How Often Does the Recurrence Score Affect Treatment? • Change in treatment recommendation by oncologist: 31% • CHT to HT 23% • Change in treatment decision by patient: 27% • CHT to HT 10% Lo SS, et al. JCO. 2010: 28: 1671
Is the Recurrence Score Assay Cost Effective? Lyman G, et al. Cancer. 109: 1011, 2007
Prospective Validation of Oncotype DX: The TAILORX Trial 11,248 ER+/LN- patients Low RS: Hormonal Therapy High RS: Chemo +Hormonal Therapy Chemo + Hormonal Hormonal Therapy Dowsett, M. & Dunbier, A. Clin Cancer Res, 2008.
Is There Concordance Between Gene Expression Profiles? 295 Stage I/II ER +/- 165 untreated 20 TAM 20 TAM + chemo 90 chemo Analyzes done with All pts & ER+ only Fan, C. NEJM, 2006.
Relapse-free Survival Overall Survival Intrinsic Subtype Recurrence Score All models except the two-gene ratio model were significant predictors of both RFS and OS. 70-Gene Profile Wound Response Two-Gene Ratio
The Molecular Portrait Hypothesis You can recognize the Mona Lisa by her smile and her nose and her eyes and even her hands – if you are really good, but not the sky or the trees
Figure 1a. Sorlie T, Tibshirani R, Parker J, et al: Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A 100:8418-23, 2003
Clinical Case 62 y/o WF with newly diagnosed IDC R breast • MMG / Ultrasound 1.2 x 1.2 cm mass at 10 o’clock + surrounding microcalcifications + several suspicious axillary LNs • s/p modified radical mastectomy • Surgical Path – 2.1 cm lesion consisting of IDC mixed with DCIS; intermediate grade; 11 (-) LNs; ER+/PR+/HER-2-; T2N0M0 • Oncotype DX - -> low risk for recurrence • Based on oncotype results her oncologist recommended adjuvant aromatase inhibitor x 5 years without chemotherapy
Conclusions • Gene signatures augment current clinicopathological variables in assessing risk of recurrence • Gene expression profiles may be both prognostic and predictive for patients with early breast cancer • NCCN guidelines suggest that Oncotype DX is an option for risk evaluation in 0.6-1 cm tumors with unfavorable characteristics or in >1 cm LN-, ER+/HER2 negative tumors
NCCN guidelines include Oncotype DX® testing in the treatment-decision pathway for node-negative and micrometastatic disease Hormone receptor-positive, HER2-negative disease pT1, pT2, or pT3 and pN1mi • Tumor 0.6-1.0 cm, moderately or poorly differentiated, intermediate or high grade, or vascular invasion • Tumor > 1 cm with favorable or unfavorable pathologic features Consider Oncotype DX No test Adjuvant endocrine therapy ± adjuvant chemotherapy RS < 18 Adjuvant endocrine therapy endocrine therapy ± adjuvant chemotherapy RS 18-30 Adjuvant Adjuvant endocrine therapy + adjuvant chemotherapy RS ≥ 31 RS, Recurrence Score® result Adapted from NCCN Practice Guidelines in Oncology – v.1.2010.
The Promise of Personalized Medicine in Breast Cancer Tamoxifen Postmenopausal Women with HR+ breast Cancer Aromatase Inhibitor Chemotherapy Anth, Taxane, Platimun Biologic agents Her2, EGFR, VEGF, Parp