Download
1 / 1
10 likes | 175 Views
A Case of Triple Hit Lymphoma. K.B. Geiersbach 1,2 , M. Sennett 3 , S.S. Shetty 1,2 1 ARUP Laboratories, 500 Chipeta Way, Salt Lake City, Utah; 2 Department of Pathology, University of Utah School of Medicine, Salt Lake City, Utah 3 Amarillo Pathology Associates, Amarillo, TX. Abstract.

E N D
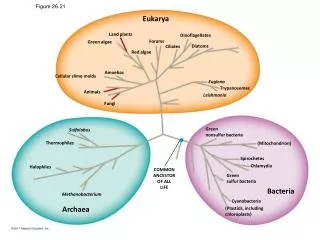
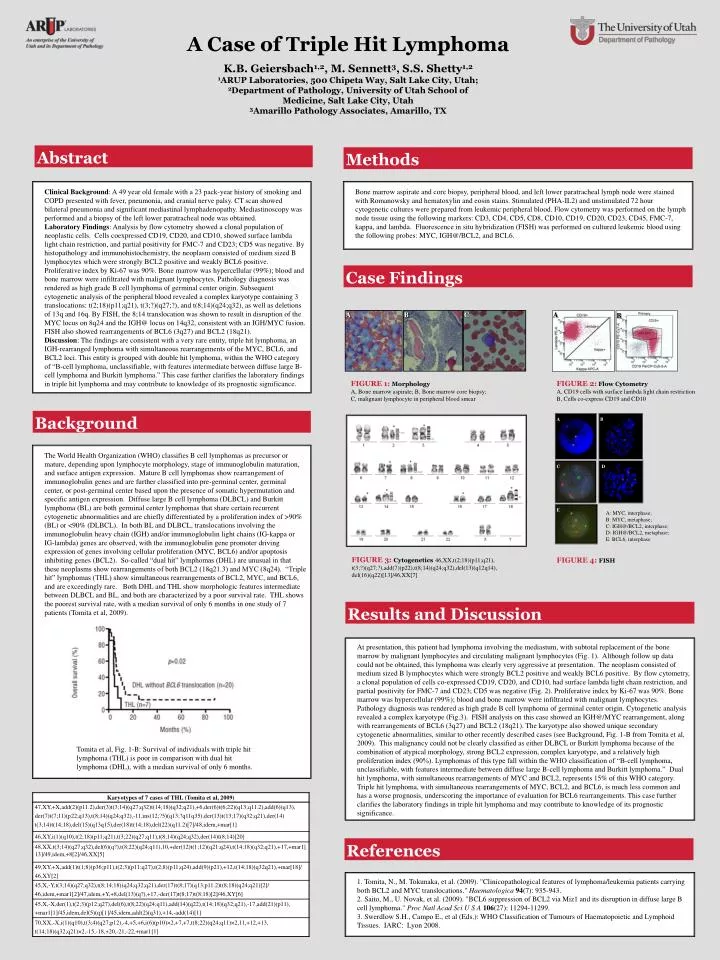
A Case of Triple Hit Lymphoma K.B. Geiersbach1,2, M. Sennett3, S.S. Shetty1,2 1ARUP Laboratories, 500 Chipeta Way, Salt Lake City, Utah; 2Department of Pathology, University of Utah School of Medicine, Salt Lake City, Utah 3Amarillo Pathology Associates, Amarillo, TX Abstract Methods • Clinical Background: A 49 year old female with a 23 pack-year history of smoking and COPD presented with fever, pneumonia, and cranial nerve palsy. CT scan showed bilateral pneumonia and significant mediastinal lymphadenopathy. Mediastinoscopy was performed and a biopsy of the left lower paratracheal node was obtained. • Laboratory Findings: Analysis by flow cytometry showed a clonal population of neoplastic cells. Cells coexpressed CD19, CD20, and CD10, showed surface lambda light chain restriction, and partial positivity for FMC-7 and CD23; CD5 was negative. By histopathology and immunohistochemistry, the neoplasm consisted of medium sized B lymphocytes which were strongly BCL2 positive and weakly BCL6 positive. Proliferative index by Ki-67 was 90%. Bone marrow was hypercellular (99%); blood and bone marrow were infiltrated with malignant lymphocytes. Pathology diagnosis was rendered as high grade B cell lymphoma of germinal center origin. Subsequent cytogenetic analysis of the peripheral blood revealed a complex karyotype containing 3 translocations: t(2;18)(p11;q21), t(3;?)(q27;?), and t(8;14)(q24;q32), as well as deletions of 13q and 16q. By FISH, the 8;14 translocation was shown to result in disruption of the MYC locus on 8q24 and the IGH@ locus on 14q32, consistent with an IGH/MYC fusion. FISH also showed rearrangements of BCL6 (3q27) and BCL2 (18q21). • Discussion: The findings are consistent with a very rare entity, triple hit lymphoma, an IGH-rearranged lymphoma with simultaneous rearrangements of the MYC, BCL6, and BCL2 loci. This entity is grouped with double hit lymphoma, within the WHO category of “B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma.” This case further clarifies the laboratory findings in triple hit lymphoma and may contribute to knowledge of its prognostic significance. • Bone marrow aspirate and core biopsy, peripheral blood, and left lower paratracheal lymph node were stained with Romanowsky and hematoxylin and eosin stains. Stimulated (PHA-IL2) and unstimulated 72 hour cytogenetic cultures were prepared from leukemic peripheral blood. Flow cytometry was performed on the lymph node tissue using the following markers: CD3, CD4, CD5, CD8, CD10, CD19, CD20, CD23, CD45, FMC-7, kappa, and lambda. Fluorescence in situ hybridization (FISH) was performed on cultured leukemic blood using the following probes: MYC, IGH@/BCL2, and BCL6. Case Findings A B C A B • FIGURE 1: Morphology • A, Bone marrow aspirate; B, Bone marrow core biopsy; • C, malignant lymphocyte in peripheral blood smear FIGURE 2:Flow Cytometry A, CD19 cells with surface lambda light chain restriction B, Cells co-express CD19 and CD10 Background A B • The World Health Organization (WHO) classifies B cell lymphomas as precursor or mature, depending upon lymphocyte morphology, stage of immunoglobulin maturation, and surface antigen expression. Mature B cell lymphomas show rearrangement of immunoglobulin genes and are further classified into pre-germinal center, germinal center, or post-germinal center based upon the presence of somatic hypermutation and specific antigen expression. Diffuse large B cell lymphoma (DLBCL) and Burkitt lymphoma (BL) are both germinal center lymphomas that share certain recurrent cytogenetic abnormalities and are chiefly differentiated by a proliferation index of >90% (BL) or <90% (DLBCL). In both BL and DLBCL, translocations involving the immunoglobulin heavy chain (IGH) and/or immunoglobulin light chains (IG-kappa or IG-lambda) genes are observed, with the immunoglobulin gene promoter driving expression of genes involving cellular proliferation (MYC, BCL6) and/or apoptosis inhibiting genes (BCL2). So-called “dual hit” lymphomas (DHL) are unusual in that these neoplasms show rearrangements of both BCL2 (18q21.3) and MYC (8q24). “Triple hit” lymphomas (THL) show simultaneous rearrangements of BCL2, MYC, and BCL6, and are exceedingly rare. Both DHL and THL show morphologic features intermediate between DLBCL and BL, and both are characterized by a poor survival rate. THL shows the poorest survival rate, with a median survival of only 6 months in one study of 7 patients (Tomita et al, 2009). C D E A: MYC, interphase; B: MYC, metaphase; C: IGH@/BCL2, interphase; D: IGH@/BCL2, metaphase; E: BCL6, interphase • FIGURE 3: Cytogenetics46,XX,t(2;18)(p11;q21), • t(3;?)(q27;?),add(7)(p22),t(8;14)(q24;q32),del(13)(q12q14), • del(16)(q22)[13]/46,XX[7] FIGURE 4: FISH Results and Discussion • At presentation, this patient had lymphoma involving the mediastum, with subtotal replacement of the bone marrow by malignant lymphocytes and circulating malignant lymphocytes (Fig. 1). Although follow up data could not be obtained, this lymphoma was clearly very aggressive at presentation. The neoplasm consisted of medium sized B lymphocytes which were strongly BCL2 positive and weakly BCL6 positive. By flow cytometry, a clonal population of cells co-expressed CD19, CD20, and CD10, had surface lambda light chain restriction, and partial positivity for FMC-7 and CD23; CD5 was negative (Fig. 2). Proliferative index by Ki-67 was 90%. Bone marrow was hypercellular (99%); blood and bone marrow were infiltrated with malignant lymphocytes. Pathology diagnosis was rendered as high grade B cell lymphoma of germinal center origin. Cytogenetic analysis revealed a complex karyotype (Fig.3). FISH analysis on this case showed an IGH@/MYC rearrangement, along with rearrangements of BCL6 (3q27) and BCL2 (18q21). The karyotype also showed unique secondary cytogenetic abnormalities, similar to other recently described cases (see Background, Fig. 1-B from Tomita et al, 2009). This malignancy could not be clearly classified as either DLBCL or Burkitt lymphoma because of the combination of atypical morphology, strong BCL2 expression, complex karyotype, and a relatively high proliferation index (90%). Lymphomas of this type fall within the WHO classification of “B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma.” Dual hit lymphoma, with simultaneous rearrangements of MYC and BCL2, represents 15% of this WHO category. Triple hit lymphoma, with simultaneous rearrangements of MYC, BCL2, and BCL6, is much less common and has a worse prognosis, underscoring the importance of evaluation for BCL6 rearrangements. This case further clarifies the laboratory findings in triple hit lymphoma and may contribute to knowledge of its prognostic significance. Tomita et al, Fig. 1-B: Survival of individuals with triple hit lymphoma (THL) is poor in comparison with dual hit lymphoma (DHL), with a median survival of only 6 months. References • 1. Tomita, N., M. Tokunaka, et al. (2009). "Clinicopathological features of lymphoma/leukemia patients carrying both BCL2 and MYC translocations." Haematologica94(7): 935-943. • 2. Saito, M., U. Novak, et al. (2009). "BCL6 suppression of BCL2 via Miz1 and its disruption in diffuse large B cell lymphoma." Proc Natl Acad Sci U S A106(27): 11294-11299. • 3. Swerdlow S.H., Campo E., et al (Eds.): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. IARC: Lyon 2008.