Download
1 / 12
130 likes | 412 Views
What is needed for diagnosis of dry eye (hint: needed to avoid staff doctor grief)?. thorough history at least one tear film assessment test TBUT w/anestetic : < 5 mm in 5 minutes aqueous deficiency w /out anesthetic: < 10 mm in 5 minutes aqueous deficiency

E N D
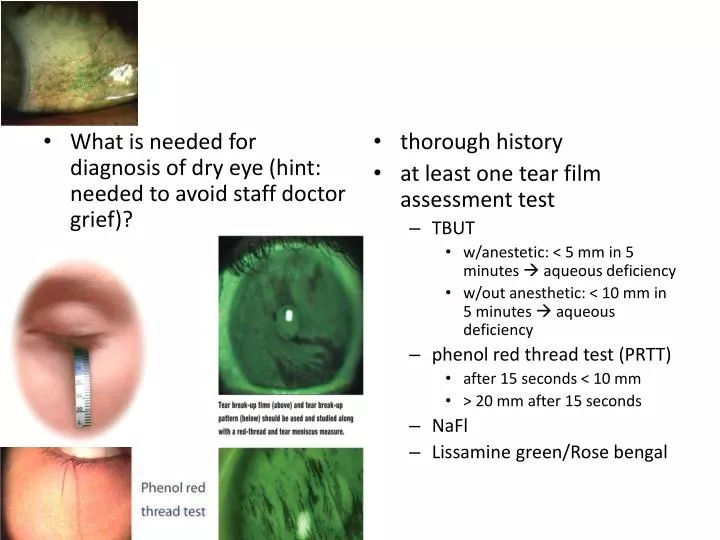
What is needed for diagnosis of dry eye (hint: needed to avoid staff doctor grief)? • thorough history • at least one tear film assessment test • TBUT • w/anestetic: < 5 mm in 5 minutes aqueous deficiency • w/out anesthetic: < 10 mm in 5 minutes aqueous deficiency • phenol red thread test (PRTT) • after 15 seconds < 10 mm • > 20 mm after 15 seconds • NaFl • Lissamine green/Rose bengal
Punctal plug management / considerations • Who typically has dry eye? • post menopausal women • Make the diagnosis & approach treatment in a methodical step-by-step fashion (if previous treatment doesn’t provide relief, proceed to next option) • artificial tears • “soft” steroids • Restasis • temporary punctal plugs (collagen) • permanent punctal plugs (silicone) • laser, cautery, lateral tarsorrhaphy
Possible complications when managing punctal plugs • canaliculitis • epiphora • dilation & irrigation (D&I) for intracanalicular • loss • patient discomfort • patient objects to cosmetic appearance (for extracanalicular)
What is dacroadenitis? • inflammation of the lacrimal gland • superior lateral eyelid and adjacent adnexa swelling • S-shaped ptosis • injection of lacrimal gland and surrounding conjunctiva • RARE!
management of dacryoadenitis (thought process) • if acute, think • viral & bacterial • if chronic, think • sarcoid, tuberculosis, Graves’, etc. • lacrimal gland tumor
management of dacryoadenitis (treatment) • oral steroids, if acute • oral antibiotics, if bacterial • Keflex 500 mg qidpo • Augmentin 875mg bid po • Levaquin 500mg qdpo (*ONLY* when patient has penicillin allergy) • palliative care, if viral • rest • ice • oral analgesics • “sounds like recognition & consult”?
differential diagnosis for epiphora • dry eye • congenital nasolacrimal duct obstruction • apositionalpunctal problem (puncta visible without lid manipulation?) • ectropion • entropion • punctal regurgitation with pressure? • atresia == congenital punctalstenosis • block in lacrimal drainage system (primary acquired nasolacrimal drainage obstruction ‘PANDO’) • aging • allergy • infection • trauma • none of above, evaluation of remainder of lacrimal system. usually monocular
evaluation of lacrimal drainage: • Jones testing: • Jones I • Jones II • Performed when Jones I is negative.
Jones I testing • NaFl in “virgin eye”; wait 5 minutes • Inspect eye for NaFl. Little to no NaFl remaining indicates “positive Jones I test.” • NaFl in back of throat, or on tissue when blowing nose confirms “positive Jones I test.” • “positive Jones I test” indicates a patentlacrimal system
Jones II testing • Indications • Negative Jones I test (significant amount of NaFl in eye after 5 minutes; AND/OR noNaFl in tissue or throat • Procedure • anesthetize punctum • dilate punctum down 2mm, in 1-2mm • insert saline-filled nasolacrimal apparatus syringe • inject 1-2mm saline • no fluid exits complete blockage surgical consult for DCR (dacryocystorhinostomy) Negative Jones II • fluid exits through upper punctum common canalicular block Negative Jones II • fluid exits through nose or patient tastes saline distal object pushed through success! Positive Jones II
describe dacryocystitis • description: • painful swelling over lacrimal sac • hyperemia • epiphora • causes • usually staph or pseudomonal related • rarely a tumor • epithelial carcinoma/lymphoma • less pain • silicone plug association • rule out • mucocele—cystic mass filled with mucous; typically arises after sinusitis; not painful
management of dacryocystitis • hot compresses & daily massage • oral antibiotic (choice & why) • dicloxicilin: 250mg qidpo • or • Levaquin: (only when pt has penicillin allergy) 500mg qdpo • 10-14 days • why? need staph/pseudomonal coverage • D&I later, after resolution • consult & culture if recalcitrant