Download
1 / 45
760 likes | 1.77k Views
Enteral Access and Tube Feeding Administration. Michele Port, P.Dt. Clinical Dietitian March 2014. Outline. Selection of the appropriate enteral access device Short-term enteral feeding tubes Long-term enteral feeding tubes Delivery systems: Open vs Closed Administration

E N D
Enteral Access and Tube Feeding Administration Michele Port, P.Dt. Clinical Dietitian March 2014
Outline • Selection of the appropriate enteral access device • Short-term enteral feeding tubes • Long-term enteral feeding tubes • Delivery systems: Open vs Closed • Administration • Case Study • Monitoring and Documentation
Learning Objectives At the end of this presentation, the participant will be able: • Determine the appropriate type of enteral access / device when assessing patients. • Understand the importance of a tube feeding protocol in advancing a tube feeding to maintenance and managing complications. • Inform medical team on appropriate method for medication administration via feeding tubes.
Selection of the Appropriate Enteral Access Device • Factors to consider: • Functional and accessible gastrointestinal tract • Normal digestion and absorption • No gastric outlet obstruction • No intestinal stricture • Gastric motility • Expected length of time enteral feeds required • Short-term (< 4 weeks) • Orogastric (intubated patients only) • Nasoenteric (nasogastric, nasoduodenal, nasojejunal) • Long-term (> 4 weeks) • Gastrostomy • Jejunostomy
Selection of the Appropriate Enteral Access Device • Aspiration risk? • Gastric vs small bowel access • Surgical intervention planned? • Tube could be placed during surgery (ex.: jejunostomy) • Patient and family preferences / activity • Pre-existing medical conditions such coagulopathy or ascites • Plan for discharge • Often rehab and long-term care facilities will only accept: • Percutaneous endoscopic gastrostomy (PEG) • Jejunostomy
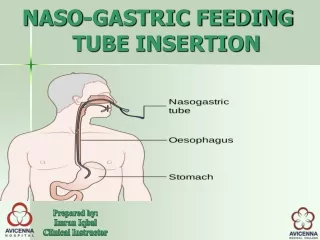
Short-Term Enteral Feeding Tubes (< 4 weeks) • Short-term use in hospitalized patients : nasogastric,nasoduodenal,nasojejunal • Pediatric IBD patients may use these tubes at home • Insertion route • Oral: in ICU post-op only with patient sedated • Nasal: Preferred route • Access • Nasogastric • Able to feed larger volumes • Large bore PVC tubes (14-18 Fr.) may be used initially but should be changed to softer more flexible tubes • PVC tubes may cause nose irritation, gastric and esophageal erosions • Not preferred access in hospitalized patients due to aspiration risk • Confirm correct feeding tube position radiographically
Short-Term Enteral Feeding Tubes (< 4 weeks) • Nasoduodenal or nasojejunal • Nasoduodenal (distal to pylorus) • Nasojejunal (distal to ligament of Treitz in jejunum) • Used when problems with delayed gastric emptying, aspiration risk, early post-op feeding (liver transplant patients malnourished pre-op) • More commonly used in non-ICU hospitalized patients • Contraindications • Obstruction head, neck, esophagus or gastric outlet obstruction
Short-Term Enteral Feeding Tubes (< 4 weeks) • Tubes : nasoduodenal or nasojejunal • Polyurethane or Silicone • Most nasoenteric tubes are made of polyurethane • Length • Varies: usually 36” (91 cm) to 60” (152 cm) • Size • Measured by external diameter in French size (Fr.) • Usually 8-12 French in adults • 10-12 Fr. commonly used due to problems with tube clogging with meds
Short-Term Enteral Feeding Tubes (< 4 weeks) • Tubes : nasoduodenal or nasojejunal • Stylet or guidewire • Provided for guiding tube insertion • Water-activated lubricant coats the inner surface of tube, needs to syringe 5-10 mL into tube before removing guidewire • Guidewire must never be reinserted, could cause perforation • Other • Tips: vary, end holes, side holes, no particular advantage • Weighted vs Unweighted tip: No advantage • Feeding connector: Y port
Short-Term Enteral Feeding Tubes (< 4 weeks) • Insertion : nasoduodenal or nasojejunal • Bedside: MD, nurse, dietitian (in certain Canadian provinces when certified) • Prokinetic agent (maxeran or erythromycin) may facilitate passage into small bowel • Endoscopic • Often tube displaced when scope removed • Fluoroscopically guided • Need to go to radiology if portable not available • Used when bedside insertion unsucessful • Surgically-placed • Often done in ENT cancer surgeries and GI surgeries where patient expected to be NPO > 1 week, malnourished pre-op, expected gastroparesis
Short-Term Enteral Feeding Tubes (< 4 weeks) • Tube position – check: • All nasogastric and nasoenteric tubes needs radiographic verification before use • With a permanent marker, mark nasal exit site • Secure tube with tape to nose
Short-Term Enteral Feeding Tubes (> 4 weeks) • Complications: nasoenteric • Insertion • Epistaxis • Respiratory compromise during tube insertion • Misplacement of tube in bronchopulmonary tree, often results in pneumothorax • Other • Tube dislodgement • Inadvertent • Patient pulls it out • Tube occlusion: Often due to medications • Tube malfunction: Kinking • Aspiration
Long-Term Enteral Feeding Tubes (> 4 weeks) Google image http://pedsurg.ucsf.edu/conditions--procedures/gastrostomy-tubes.aspx
Long-Term Enteral Feeding Tubes (> 4 weeks) • Placement techniques • Surgically: open gastrostomy, jejunostomy • Endoscopically(sedation, local anesthetic) • Percutaneous endoscopic gastrostomy (PEG) • Percutaneous transgastric jejunostomy (PEG/J) • Radiologically • Radiologically inserted gastrostomy • Radiologically inserted transgastric jejunostomy • Radiologically inserted jejunostomy – rarely done at my center.
Long-Term Enteral Feeding Tubes (> 4 weeks) • Size • Gastrostomies: usually 18-28 Fr., average 22 French • Jejunostomies: 8-14 Fr. • Internal and external bolster or bumper (silicone or polyurethane) and/or balloon (silicone) of PEG • Balloons have lifespan of 3-4 months • Ports • Usually a port for feeding and a port for medication • PEG/J: Percutaneous endoscopic gastrostomy with jejunal extension • 3 ports: • Bal. = Balloon • Jejunal = Feed • Gastric
Long-Term Enteral Feeding Tubes (> 4 weeks) • Peristomal Care • Clean area with mild soap and water • Dressings are not needed unless there is drainage at site • Complications • Aspiration during procedure • Hemorrhage • Peritonitis • Pneumoperitoneum • Peristomal infection • Accidental tube removal • If stoma tract mature put foley in to keep open until tube replaced • Buried bumper syndrome: Gastric mucosa grows over internal bumper • Clogging
Long-Term Enteral Feeding Tubes (> 4 weeks) • Replacement as per manufacturer’s recommendation and hospital policy • Removal of PEG • Only after tract has matured, after 4 weeks • If on steroids, after 6 weeks • Some contraindications to PEG • Ascites • Extensive gastric ulceration • Gastric varices • Coagulopathy • Morbid obesity
Long-Term Enteral Feeding Tubes (> 4 weeks) • Practice recommendations for long-term enteral device placement include: • Document tube type, tip location and external markings in medical record and on follow-up • Avoid placement of catheters or tubes not intended for use as feeding devices such as foleys • Evaluation by multidisciplinary team prior to insertion of long-term feeding device
Delivery Systems: Open vs. Closed CLOSED feeding system OPEN feeding system Google images www.dhphomedelivery.com www.berktree.com www.abbott.ca
Nursing practice for monitoring of enteral feeding Care of Open Feeding System • Use disposable gloves during the administration of TF. • Label each container with patient’s name, date, time of first use, and formula’s name. • Wipe top of formula container with damp paper towel before opening. • Do not add anything to the container other than the formula. • Fill container with maximum of 4 hours of the feeding formula. • Rinse container and tube well q 4 hours with water for continuous feedings or after each intermittent feedings. • Change administration sets for open tube feeds every 24 hours. • Discard any opened or mixed formula after 24 hours. • Store unopened commercial liquid tube feeding (TF) formulas under controlled (dark, dry, cool) conditions.
Nursing practice for monitoring of enteral feeding Care of Closed Feeding System • Use disposable gloves during the administration of TF. • Label container along with patient’s name, date, and time when container was spiked. • Shake feeding bag well for 10 seconds when starting, then every 4 hours. • Do not add anything to the container. • Closed-system TF formulas can hang for 48 hours as per manufacturer’s guidelines. • Change administration set each time formula container is changed. • Discard any unused formulas and spike set after 48 hours. • Refer to product information sheet for further detail. • Store unopened commercial liquid tube feeding (TF) formulas under controlled (dark, dry, cool) conditions.
Nursing practice for monitoring of enteral feeding • Choice of system: • Product availability • Preference of patient and family
Administration PUMPS Pumpsneeds to be calibrated periodically to assess accuracy. • Small, portable with battery for 4-8 hours • Pumps in back-pack for home use • Feed and flush pumps • Will automatically flush tube as programmed • Quantify feeding provided
Administration • Positioning: • Important to GER and possible aspiration • Practice recommendations: • HOB to a minimum of 30⁰ (preferably 45⁰), for all patients on EN, unless medically contraindicated • Use reverse trendelenberg position if HOB can't be elevated, unless medically contraindicated • If head of bed must be lowered for a procedure, return patient to elevated HOB position Bankhead et al. JPEN 2009, Boullata, J et al. eds. A.S.P.E.N. Enteral Nutrition handbook. ASPEN 2010 • Water flushes • For hydration and cleaning of tube • Use sterile water in immunocompromised and critically ill • Medication administration
Administration • Oral Hygiene • Poor oral / dental hygiene can increase bacteria in oral secretions risk for aspiration pneumonia • Need tooth brushing / mouth wash twice per day
Administration of Medications • Use oral route if safe / possible. • Check with pharmacy if uncertain which medications can be delivered by tube and/or the appropriate delivery method. • Never add medication directly to an enteral feeding formula. • Never mix medications together (to avoid chemical incompatibilities, tube obstruction…) • Dilute medications appropriately prior to administration: • Use liquid forms when available. • Grind simple compressed tablets to a fine powder and mix with 30 mL water. • Dilute viscous liquids with 15-30 mL water and concentrated liquids with 30-60 mL water. • Do not crush slow release tablets or enteric coated tablets. • Open hard gelatin capsules and mix contents with water.
Administration of Medications • Prior to administering medication, stop feeding and flush the tube with 30 mL water. • Administer each medication separately and flush the tube with at least 30 mL of water after each medication. • Use sterile water for immunocompromisedpatients. • Start with liquid medications, followed by those that have been diluted. Keep viscous medications until the end. • Rinse the tube one final time with 30 mL water. • Record the volume of water given on the input/output sheets. • In the case of continuous feeding, resume formula administration immediately unless contraindicated as in the case of drug-nutrient interaction.
Administration • Drug nutrient interactions • Many possible drug - nutrient interactions. Boulatta et al. 2010
Enteral feeding protocol • After nutrition assessment, caloric and protein requirements are calculated. • If Na, K, phosphorus or fluid is limited i.e.: in case of dialysis patients this must also be taken in consideration.
Monitoring and Documentation of Enteral Feeding Administration Following tube placement verification by x-ray, mark exit point of tube. Confirm HOB elevation at 30o – 45o, unless medically contraindicated. Observe and document any signs of intolerance such as abdominal distension, firmness, discomfort, nausea, vomiting, or diarrhea. Notify and consult the Clinical Dietitian and MD of any of these feeding intolerances and interruptions. Ensure adequate mouth care. Document GRV for gastrically fed patients in progress notes. Verify placement of feeding tube q 8 hours, prn. Weigh patient on day 1 of tube feeding, then every 1-7 day(s). Enter data in OACIS. Document volume delivered for each tube flush. Document the volume of formula delivered each shift including the volume of any modular product also delivered (ex., protein powder) if needed.
Preventing Feeding Tube Blockage • Possible causes include inadequate tube irrigation, administering improperly crushed medication, intraluminal accumulation of formula residue, solidification of formula, medication residue. To prevent feeding tube blockage: • Immediately flush the feeding tube with a minimum of 30 mL of water after each feeding, after administration of each medication, after any interruption in feeding. • Shake the enteral feeding container before hanging for 10 seconds. • Shake formula every 4 hours (i.e. when flushing the tubing). • Change the feeding bag and tubing used for enteral feeding every 24 hr for the open system and every 48 hr for the closed system. • Use liquid formulations of medications whenever possible. • Unless contraindicated, crush solid medications thoroughly. • Use a syringe (60 mL) filled with 30 ml water to flush the tube before and after administering medications. Replace syringe every 24 hours. • Rinse using 30 ml water after measuring gastric residual volume. • Use a feeding pump.
Unblocking of Obstructed Feeding Tubes • Possible Causes: • Inadequate irrigation of tube. • Administration of improperly crushed medication, intraluminal accumulation of formula residue, solidification of formula or medication residue because of drug/nutrient interaction. • Improperly dissolved enteral formula due to poor mixing technique
Unblocking of Obstructed Feeding Tubes • Prevention: • Immediately flush the feeding tube with a minimum of 30 mL of water after each feeding, after administration of each medication, after any interruption in feeding. • Shake the enteral feeding container before hanging for 10 seconds. • Shake formula regularly (i.e. every 8 hours or when flushing the tubing). • Change the feeding bag and tubing used for enteral feeding every 24 hr for the open system and every 48 hr for the closed system. • Use liquid formulations of medications whenever possible. • Unless contradicted, crush solid medications thoroughly. • Use a syringe (60 mL) filled with 30 ml water to flush the tube before and after administering medications. Replace syringe very 24 hours. • Rinse using 30 mL of water after measuring gastric residual volume. • Use a feeding pump equipped with a flush feature. Schedule flushes q 4h.
Unblocking of Obstructed Feeding Tubes • Treatment as per MD’s orders. • In order to restore tube patency, first flush with warm water. • If this is ineffective: • Dissolve one 500 mg crushed tablet of sodium bicarbonate in 5-10 mL sterile water (this will take about 3-5 minutes). • Once dissolved, mix contents of 1 opened capsule of pancreatic enzyme, Cotazym ECS20, into the sodium bicarbonate / water mix, allow to dissolve 5 minutes, the mixture should turn a light brown color. • Suspend mixture by adding 15 mL of warm water. • Introduce the pancreatic enzyme solution into the feeding tube while gently massaging the tube. • Clamp the tube and leave the pancreatic enzyme solution in the tube for 30 minutes before flushing the tube. • Repeat the above once if necessary. Contact MD in event of failure.
Unblocking of Obstructed Feeding Tubes • NEVER USE Cranberry juice or carbonated beverages such as cola as their acidity may aggravate the blockage. • NEVER try to restore patency of a feeding tube by reinserting the stylet because of the risk of intestinal perforation.
Monitoring • Monitoring and documentation of enteral feed administration (nurse, dietitian) • Monitoring by team to prevent and correct complications • Adequacy of nutritional intake • Physical assessment ex.: check for edema • GI tolerance: • Stool frequency / consistency • Ostomy output • Abdominal distension / pain • Nausea and vomiting • Residual volumes: look for change • Glycemic control
Monitoring • Fluid intake and output • Weight (1 x per week): look at trend • Lab data • Markers of nutrition adequacy if applicable (include CRP) • Review medications • Medical procedures which require discontinuation of feeding
Conclusion There are many enteral access devices to choose from. It is important to communicate to the patient and family (if possible) why you recommend a specific device i.e: PEG vs PEG/J. The best way to ensure enteral feeding safety is to implement enteral nutrition practice guidelines such as those from ASPEN or ESPEN, educate all staff and then audit to see if those guidelines are being followed.
References Bankhead R, Fang J. Enteral Access Devices. In Gottschlich P, ed. in chief. The A.S.P.E.N. Nutrition Support Core Curriculum, Silver Spring, MD. 2007; 233-245. Bankhead R, Boullatta J, Brantley S, et al and the A.S.P.E.N. Board of Directors, Enteral nutrition practice recommendations. JPEN 2009; 33; 122-167. Boullata J, Nieman Carney L, Guenter P, eds. A.S.P.E.N. Enteral Nutrition Henadbook. Silver Spring, MD. A.S.P.E.N. 2010. Shroud M, Duncan H, Nightingale J. Guidelines for enteral feeding in adult hospital patients Gut 2003; 52 (Suppl VII); vii1-vii12. MUHC Adult Sites. Interprofessional Professional protocol for the initiation and monitoring of enteral feedings. 2013