Download
1 / 17
170 likes | 350 Views
Cardiovascular Anatomy-Histology Correlate. By: Michael Lu, Class of ‘07. NOTE: Visceral pleura is in direct contact with the lungs, while parietal pleura is everything else. The same applies to pericardium and the heart.

E N D
CardiovascularAnatomy-Histology Correlate By: Michael Lu, Class of ‘07
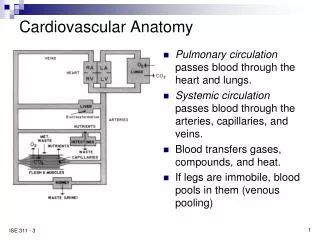
NOTE: • Visceral pleura is in direct contact with the lungs, while parietal pleura is everything else. The same applies to pericardium and the heart. • 4 sections of parietal pleura: cupola, costal, diaphragmatic, and mediastinal. • Potential spaces of the costomediastinal and costodiaphragmatic recesses, where there is no lung tissue. • Mediastinum located between the lungs extending from the sternum anteriorly to vertebrae posteriorly. • a) superior – bounded by horizontal line through sternal angle below and rib 1 above • b) anterior – bounded by sternum in front and pericardium in back • c) middle – includes heart and pericardium • d) posterior – bounded by pericardium in front and vertebral bodies in back; includes esophagus and aorta • Phrenic nerves (right and left) – motor nerves to diaphragm that travel along the side of the heart in the pericardium in front of the root of the lung • Pericacardiacophrenic arteries and veins traveling with the phrenic nerves. • Thymus gland – immune tissue, becomes fatty tissue with age Heart in Situ
Heart – Anterior Pericardial Sac Removed • NOTE: • The superior vena cava, aortic arch, and pulmonary trunk exiting the base of the heart. • The internal and external jugular veins joining the subclavian vein to become the brachiocephalic veins that drain into the superior vena cava. • Since the superior vena cava is on the right, the left brachiocephalic vein is longer than the right brachiocephalic vein and crosses midline. • The aorta bending left and inferiorly, its arch giving off 3 main branches: • a) brachiocephalic trunk, which gives off right subclavian and right common carotid arteries • b) left common carotid artery directly off aorta • c) left subclavian artery directly off aorta • The veins are situated anterior to the arteries. • The pulmonary trunk giving off right and left pulmonary arteries to the lungs. • Ligamentum arteriosum attached between the aortic arch and left pulmonary artery. • Vagus n. running in the mediastinum behind the lung root, giving off the recurrent laryngeal n. on the left side under the aortic arch. • Right ventricle of the heart is situated most anterior and the apex is left of midline.
NOTE: • With the heart removed, the openings of the great vessels at the base of the heart: superior and inferior vena cava, pulmonary trunk bifurcating into left and right pulmonary arteries, left and right pulmonary veins, and ascending aorta. • Once again, the phrenic nerves running anterior to the roots of the lungs and the vagus nerves (not shown here) running posterior. • The transverse pericardial sinus situated behind the pulmonary trunk and ascending aorta (easily felt by inserting a finger from behind these great vessels from the left with heart in situ). • The oblique pericardial sinus behind the diaphragmatic surface up to the base of the heart (easily felt by lifting the apex and sliding fingers behind the heart). • Throughout the cardiovascular system, like all other organ systems in the body, structure correlates with function. This is true from the heart all the way down to the capillary. In the following slides, we will look closely at the histological details of arteries and veins, starting with the great vessels.
AORTA (intima) • All vessel walls are divided into 3 tunica (starting from inside): intima, media, and adventitia. • The inner intima layer consists of simple squamous epithelium and underlying connective tissue. • The border between the tunica intima and tunica media may not be easy to recognize. As a general rule of thumb, the intima ends and the media begins where the first distinct elastic sheet or lamella is located. • In the figure below, the elastic sheet is indicated by arrowheads, and the intima is indicated by the bracket.
Thickening of Tunica Intima Thickening of the tunica intima may occur in 2 ways – arteriosclerosis and atherosclerosis. Arteriosclerosis is a part of normal aging. There is an increase in connective tissue, fibrosis, and fragmentation of elastic lamellae. Atherosclerosis, on the other hand, is a pathological process involving eccentric fibrous intimal thickening, lipid deposition, and dystrophic calcification. Intima thickening within coronary arteries, which nourish the myocardium of the heart, is a major cause for myocardial infarcts. Shown below are examples of tunica intima thickening. As a reminder, the presence of elastic lamellae, or in this case a distinct internal elastic membrane, separates the tunica intima from the tunica media.
AORTA (media) • The tunica media consists of circularly arranged smooth muscle and abundant elastic tissue. In the H&E stain below, the arrows point to a smooth muscle cell nucleus and elastic lamella (E). • The Masson-aldehyde fuchsin stain accentuates the abundance of elastic lamellae within the tunica media. • The smooth muscle cells, not fibroblasts, synthesize the elastic fibers, in addition to collagen and various proteoglycans.
AORTA (adventitia) • The outermost layer of the vessel wall, the tunica adventitia, is mainly a connective tissue sheath surrounding the vessel. • The media ends and adventitia begins where the elastic lamellae are not found. • The H&E stain below shows the border between the media and adventitia. In larger vessels, such as the aorta in this case, the adventitia contains small arteries and veins, also called vasa vasorum, and their smaller branches (arrowheads) that supply nourishment to the outer half of the media.
Comparison of Artery and Vein • There are several criteria that can help you distinguish • between arteries and veins. • Arteries experience a much higher blood pressure than veins and therefore have a much higher wall-to-lumen ratio (structure correlates with function). On the other hand, venous pressure is much lower and thus veins have a lower wall-to-lumen ratio, or wider lumen and thin wall. • Veins are more variably shaped than arteries. • Most arteries contain a distinct internal elastic membrane (labeled as iem), while veins do not. • In an artery, the media is thicker than the adventitia. Once again, the media contains abundant smooth muscle and elastic fibers. The adventitia does not contain any muscle. • In a vein, the adventitia is thicker than the media. The media consists of circumferentially oriented smooth muscle fibers, while the adventitia contains longitudinal smooth muscle fibers. The adventitia is the thickest layer. Adventitia of vein
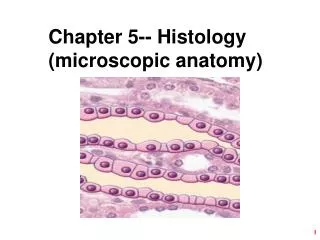
NOTE: • The heart serves as a mechanical pump to supply the entire body with blood, both providing nutrients and removing waste products. • The great vessels exit the base of the heart. • Blood flow: body→vena cava→right atrium→right ventricle→lungs→left atrium→left ventricle→body • The heart consists of 3 layers – the endocardium, myocardium, and epicardium. The epicardium (bottom left) consists of arteries, veins, nerves, connective tissue, and variable amounts of fat. • The myocardium contains branching, striated muscle cells with centrally located nuclei. They are connected by intercalated disks (arrowheads).
Coronary arteries and cardiac veins supply the muscular tissue of the heart. The left and right coronary arteries immediately branch off of the ascending aorta and further give off the left anterior descending (LAD), circumflex, SA nodal, right marginal, posterior descending, and atrial branches. • The small cardiac, middle cardiac, and great cardiac veins all drain into the coronary sinus, which wraps around the heart and drains into the right atrium. • The following slide details the 4 chambers of the heart – left and right atria and ventricles. Two features to notice are the fossa ovalis and the ligamentum arteriosum, which are remnants of shunts that were open during circulation through the fetal heart in order to bypass the lungs.
Endocardium of Atrium and Ventricle • These sections of heart are both taken near the atrio-ventricular sulcus that contains a coronary artery and cardiac vein. They also exhibit all 3 layers of the heart wall – epicardium, myocardium, and endocardium. • Notice (both here and in the previous slide) that the myocardium in the ventricle is much thicker than that in the atrium. • The endocardium (marked by the black bracket) is magnified in the lower panel and compared between the atrium and the ventricle. • The atrial endocardium is much thicker than the ventricular endocardium and contains a well-developed network of elastic fibers. • Right beneath the ventricular endocardium are conducting fibers that will be covered in the next 2 slides.
Conducting System of the Heart • The heart continuously pumps blood to the entire body without input from elsewhere. • Nerve impulses initiate from the sinoatrial (SA) node and travel down to the atrioventricular (AV) node. They continue down the bundle of His and spread out among the Purkinje fibers towards the apex of the heart. This mechanism provides regular, synchronous contractions of the myocardium. • The Purkinje fibers can be found immediately beneath the endocardium of the ventricular papillary muscle or in other regions immediately underneath the ventricular endocardium. • The Purkinje conducting fibers are modified cardiac muscle cells, specialized for the conduction of electrochemical impulses. They appear much larger and paler than cardiac muscle fibers. • The square near the left bundle is enlarged in the next slide.
This section was taken near the interventricular septum. The nerve tissue of the AV bundle, or bundle of His (lighter staining enclosed in bracket), must travel through the cardiac skeleton down a small fascicle of muscle fibers. The nerve fibers then travel down the interventricular septum towards the apex of the heart as Purkinje fibers. • The cardiac skeleton consists of dense connective tissue surrounding the cardiac valves, on which all the muscle fibers of the heart insert. When the cardiac muscles contract, they pull toward these insertion points and empty the atria and ventricles.
Cardiac Valves • As shown in the previous slide, the heart contains 4 valves – the tricuspid, pulmonary, mitral, and aortic valves. The valves prevent regurgitation of blood flow. • The cardiac valves are essentially plates of dense connective tissue extending from the cardiac skeleton covered with endothelium. They are avascular. • The side of the valve that faces oncoming blood flow exhibits an extensive elastic fiber network. As the blood is squeezed out of the heart chamber, the increased blood pressure pushes the valve open. As the blood flows past the valve and the pressure drops, the elastic fibers recoil and help the valve to close. The other side of the valve contains abundant collagen fibers. • Both atrial valves, the tricuspid and mitral valves, are attached to papillary muscles in the ventricles via chordae tendineae. The papillary muscles and chordae tendineae do NOT pull open the valves. All valves open and close passively. Instead, these structures hold the tricuspid and mitral valves shut to prevent regurgitation of blood back into the atria when the ventricles contract. The blood exits the ventricles via the pulmonary and aortic valves.