Download
1 / 1
10 likes | 117 Views
A case series of XY females in the first Malaysian PAG clinic NurZaireena Z.,* Amelia A.Z., * NurAzurah A.G., ***S. R. Grover, ** Suraya Aziz,* Sharul Rizal Samsury , * Z. A. Mahdy

E N D
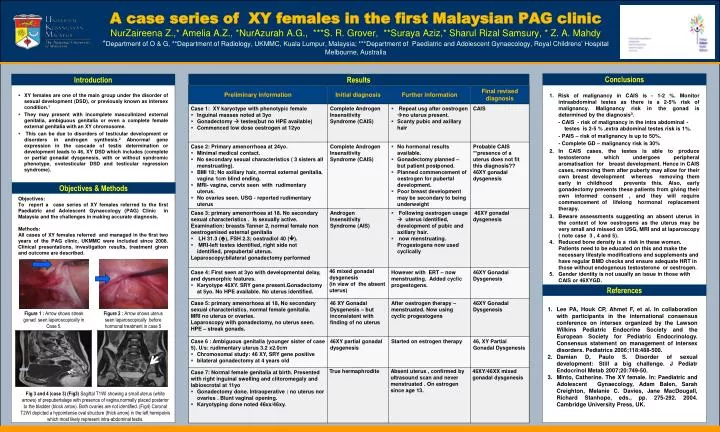
A case series of XY females in the first Malaysian PAG clinic NurZaireena Z.,* Amelia A.Z., *NurAzurah A.G., ***S. R. Grover, **Suraya Aziz,* Sharul Rizal Samsury, * Z. A. Mahdy *Department of O & G, **Department of Radiology, UKMMC, Kuala Lumpur, Malaysia; ***Department of Paediatric and Adolescent Gynaecology, Royal Childrens’ Hospital Melbourne, Australia Conclusions Introduction Results • XY females are one of the main group under the disorder of sexual development (DSD), or previously known as intersex condition.1 • They may present with incomplete masculinized external genitalia, ambiguous genitalia or even a complete female external genitalia with an XY chromosome. • This can be due to disorders of testicular development or disorders in androgen synthesis.2 Abnormal gene expression in the cascade of testis determination or development leads to 46, XY DSD which includes (complete or partial gonadaldysgenesis, with or without syndromic phenotype, ovotesticular DSD and testicular regression syndrome). • Objectives: • To report a case series of XY females referred to the first Paediatric and Adolescent Gynaecology (PAG) Clinic in Malaysia and the challenges in making accurate diagnosis. • Methods: • All cases of XY females referred and managed in the first two years of the PAG clinic, UKMMC were included since 2008. Clinical presentations, investigation results, treatment given and outcome are described. • 1. Risk of malignancy in CAIS is - 1-2 %. Monitor intraabdominal testes as there is a 2-5% risk of malignancy. Malignancy risk in the gonad is determined by the diagnosis3. • - CAIS - risk of malignancy in the intra abdominal - testes is 2-5 % ,extra abdominal testes risk is 1%. • - PAIS – risk of malignancy is up to 50%. • - Complete GD – malignancy risk is 30% • In CAIS cases, the testes is able to produce testosterone which undergoes peripheral aromatisation for breast development. Hence in CAIS cases, removing them after puberty may allow for their own breast development whereas removing them early in childhood prevents this. Also, early gonadectomy prevents these patients from giving their own informed consent , and they will require commencement of lifelong hormonal replacement therapy. • Beware assessments suggesting an absent uterus in the context of low oestrogens as the uterus may be very small and missed on USG, MRI and at laparoscopy ( note case 3 , 4 and 5). • 4. Reduced bone density is a risk in these women. Patients need to be educated on this and make the necessary lifestyle modifications and supplements and have regular BMD checks and ensure adequate HRT in those without endogenous testosterone or oestrogen. • 5. Gender identity is not usually an issue in those with CAIS or 46XYGD. Objectives & Methods References • Lee PA, Houk CP, Ahmet F, et al. In collaboration with participants in the international consensus conference on intersex organized by the Lawson Wilkins Pediatric Endocrine Society and the European Society for Pediatric Endocrinology. Consensus statement on management of intersex disorders. Pediatrics 2006;118:488-500. • Damian D, Paulo S. Disorder of sexual development: Still a big challenge. J PediatrEndocrinolMetab 2007;20:749-50. • Minto, Catherine. The XY female. In: Paediatric and Adolescent Gynaecology, Adam Balen, Sarah Creighton, Melanie C. Davies, Jane MacDougall, Richard Stanhope, eds., pp. 275-292. 2004. Cambridge University Press, UK. Figure 1 : Arrow shows streak gonad seen laparoscopically in Case 5. Figure 2 : Arrow shows uterus seen laparoscopically before hormonal treatment in case 5 Fig 3 and 4 (case 3) (Fig3) Sagittal T1WI showing a small uterus (white arrows) of prepubertalage with presence of vagina,normally placed posterior to the bladder (block arrow). Both ovaries are not identified. (Fig4) Coronal T2WI depicted a hypointense oval structure (thick arrow) in the left hemipelvis which most likely represent intra-abdominal testis.






