Download
1 / 1
10 likes | 186 Views
Does low cord blood pH gasses determines fetal outcome? Dr. Ahmad Tayyib Azizan, Dr. H. Krishna Kumar Tuanku Jaa’far Seremban Hospital, Negeri Sembilan Darul Khusus, Malaysia. Methods. Results. Objectives. Conclusions.

E N D
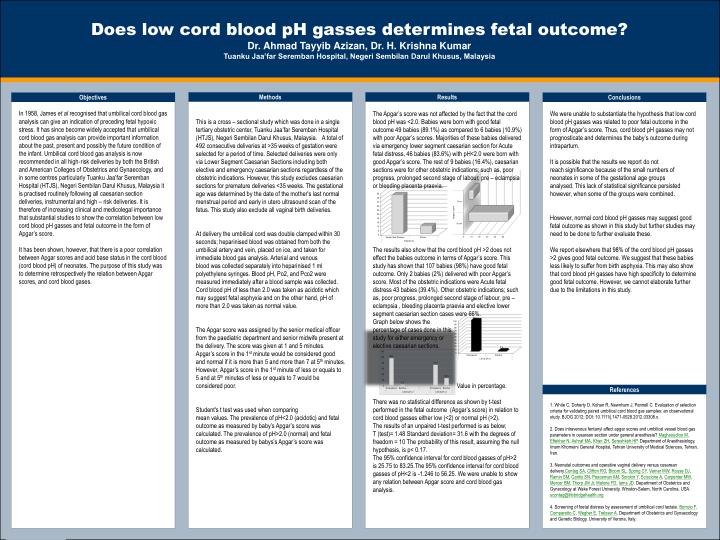
Does low cord blood pH gasses determines fetal outcome? Dr. Ahmad Tayyib Azizan, Dr. H. Krishna Kumar Tuanku Jaa’far Seremban Hospital, Negeri Sembilan Darul Khusus, Malaysia Methods Results Objectives Conclusions In 1958, James et al recognised that umbilical cord blood gas analysis can give an indication of preceding fetal hypoxic stress. It has since become widely accepted that umbilical cord blood gas analysis can provide important information about the past, present and possibly the future condition of the infant. Umbilical cord blood gas analysis is now recommended in all high‐risk deliveries by both the British and American Colleges of Obstetrics and Gynaecology, and in some centres particularly Tuanku Jaa’far Seremban Hospital (HTJS), Negeri Sembilan Darul Khusus, Malaysia it is practised routinely following all caesarian section deliveries, instrumental and high – risk deliveries. It is therefore of increasing clinical and medicolegal importance that substantial studies to show the correlation between low cord blood pH gasses and fetal outcome in the form of Apgar’s score. It has been shown, however, that there is a poor correlation between Apgar scores and acid base status in the cord blood (cord blood pH) of neonates. The purpose of this study was to determine retrospectively the relation between Apgar scores, and cord blood gases. This is a cross – sectional study which was done in a single tertiary obstetric center, Tuanku Jaa’far Seremban Hospital (HTJS), Negeri Sembilan Darul Khusus, Malaysia. A total of 492 consecutive deliveries at >35 weeks of gestation were selected for a period of time. Selected deliveries were only via Lower Segment Caesarian Sections including both elective and emergency caesarian sections regardless of the obstetric indications. However, this study excludes caesarian sections for premature deliveries <35 weeks. The gestational age was determined by the date of the mother's last normal menstrual period and early in utero ultrasound scan of the fetus. This study also exclude all vaginal birth deliveries. At delivery the umbilical cord was double clamped within 30 seconds; heparinised blood was obtained from both the umbilical artery and vein, placed on ice, and taken for immediate blood gas analysis. Arterial and venous blood was collected separately into heparinised 1 ml polyethylene syringes. Blood pH, Po2, and Pco2 were measured immediately after a blood sample was collected. Cord blood pH of less than 2.0 was taken as acidotic which may suggest fetal asphyxia and on the other hand, pH of more than 2.0 was taken as normal value. The Apgar score was assigned by the senior medical officer from the paediatric department and senior midwife present at the delivery. The score was given at 1 and 5 minutes. Apgar’s score in the 1st minute would be considered good and normal if it is more than 5 and more than 7 at 5th minutes. However, Apgar’s score in the 1st minute of less or equals to 5 and at 5th minutes of less or equals to 7 would be considered poor. Student's t test was used when comparing mean values. The prevalence of pH<2.0 (acidotic) and fetal outcome as measured by baby’s Apgar’s score was calculated. The prevalence of pH>2.0 (normal) and fetal outcome as measured by babys’s Apgar’s score was calculated. • The Apgar’s score was not affected by the fact that the cord blood pH was <2.0. Babies were born with good fetal outcome 49 babies (89.1%) as compared to 6 babies (10.9%) with poor Apgar’s scores. Majorities of these babies delivered via emergency lower segment caesarian section for Acute fetal distress, 46 babies (83.6%) with pH<2.0 were born with good Apgar’s score. The rest of 9 babies (16.4%), caesarian sections were for other obstetric indications; such as, poor progress, prolonged second stage of labour, pre – eclampsia or bleeding placenta praevia. • The results also show that the cord blood pH >2 does not effect the babies outcome in terms of Apgar’s score. This study has shown that 107 babies (98%) have good fetal outcome. Only 2 babies (2%) delivered with poor Apgar’s score. Most of the obstetric indications were Acute fetal distress 43 babies (39.4%). Other obstetric indications; such as, poor progress, prolonged second stage of labour, pre – eclampsia , bleeding placenta praevia and elective lower segment caesarian section cases were 66%. • Graph below shows the • percentage of cases done in this • study for either emergency or • elective caesarian sections. • Value in percentage. • There was no statistical difference as shown by t-test performed in the fetal outcome (Apgar’s score) in relation to cord blood gasses either low (<2) or normal pH (>2). • The results of an unpaired t-test performed is as below; • T (test)= 1.48 Standard deviation= 31.6 with the degrees of freedom = 10 The probability of this result, assuming the null hypothesis, is p< 0.17. • The 95% confidence interval for cord blood gasses of pH>2 is 25.75 to 83.25.The 95% confidence interval for cord blood gasses of pH<2 is -1.246 to 56.25. We were unable to show any relation between Apgar score and cord blood gas analysis. We were unable to substantiate the hypothesis that low cord blood pH gasses was related to poor fetal outcome in the form of Apgar’s score. Thus, cord blood pH gasses may not prognosticate and determines the baby’s outcome during intrapartum. It is possible that the results we report do not reach significance because of the small numbers of neonates in some of the gestational age groups analysed. This lack of statistical significance persisted however, when some of the groups were combined. However, normal cord blood pH gasses may suggest good fetal outcome as shown in this study but further studies may need to be done to further evaluate these. We report elsewhere that 98% of the cord blood pH gasses >2 gives good fetal outcome. We suggest that these babies less likely to suffer from birth asphyxia. This may also show that cord blood pH gasses have high specificity to determine good fetal outcome. However, we cannot elaborate further due to the limitations in this study. References 1. White C, Doherty D, Kohan R, Newnham J, Pennell C. Evaluation of selection criteria for validating paired umbilical cord blood gas samples: an observational study. BJOG 2012; DOI: 10.1111/j.1471-0528.2012.03308.x. 2. Does intravenous fentanyl affect apgar scores and umbilical vessel blood gas parameters in cesarean section under general anesthesia? Maghsoudloo M, Eftekhar N, Ashraf MA, Khan ZH, Sereshkeh HP. Department of Anesthesiology, Imam Khomeini General Hospital, Tehran University of Medical Sciences, Tehran, Iran. 3. Neonatal outcomes and operative vaginal delivery versus cesarean delivery.Contag SA, Clifton RG, Bloom SL, Spong CY, Varner MW, Rouse DJ, Ramin SM, Caritis SN, Peaceman AM, Sorokin Y, Sciscione A, Carpenter MW, Mercer BM, Thorp JM Jr, Malone FD, Iams JD. Department of Obstetrics and Gynecology at Wake Forest University, Winston-Salem, North Carolina, USA. scontag@lifebridgehealth.org 4. Screening of foetal distress by assessment of umbilical cord lactate. Borruto F, Comparetto C, Wegher E, Treisser A. Department of Obstetrics and Gynaecology and Genetic Biology, University of Verona, Italy.