Download
1 / 31
310 likes | 466 Views
Grades. Exam and quiz scores are posted, Roughly alphabetical, (WWU#). Please check for accuracy, Extra Credit (not yet compiled), Seminars, Paper, odds and ends to be posted by Tuesday. Email Extra Credit.

E N D
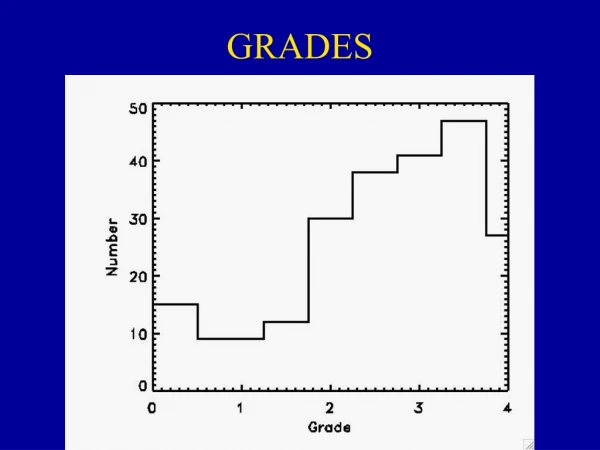
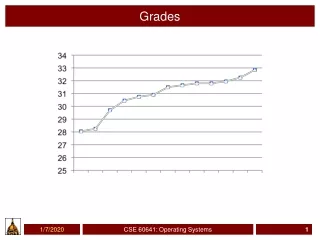
Grades • Exam and quiz scores are posted, • Roughly alphabetical, (WWU#). • Please check for accuracy, • Extra Credit (not yet compiled), • Seminars, Paper, odds and ends to be posted by Tuesday.
Email Extra Credit • Your email extra credits (through 8 AM, June 7th) are posted. I’ll count the entries as listed. • If you placed more than one synopsis in an email, please put a star, or a mark by your name. • Remember, you were instructed to send no more than one article per email. Note: some of you emailed the MCK paper. That’s OK, I have both hard and soft copies.
Points • Please don’t panic over a few points, • If you are close to a grade break, and have done a significant amount of extra credit, you’ll definitely get the benefit of the doubt.
Final • Total point value is 100, • I’ll grade both sections on a 100% scale, and convert the totals to 100 pts.
Chapter Self Study Questions, • Two ways to get a right answer, • Best: get it right. • Just about as good (probably equal in points to a right answer), • Explain why you can’t answer the problem, suggest alternative approaches that you’ve considered, or make an assumption and answer it based on the assumption.
Due Tuesday, 4 PM(my office box BI315) • I’ll be in my office during the scheduled final hours, • Tuesday, 10:30 - 12:30.
Hereditary Fructose Intolerance • Fructose intolerance was first noted in severely ill infants with recurrent hypoglycemia (low blood sugar) and vomiting, occurring at the time of weaning when fructose or sucrose is added to the diet and resulting in marked malnutrition. • However, a 3-year-old brother of a severely affected infant was found to have hepatomegaly (enlarged liver), and hypoglycemic shock was precipitated by an oral test dose of fructose, although he was clinically healthy. He had a marked aversion to sweets and fruit. • Subsequently,2 adults, aged 33 and 39 years were identified with the same condition . In addition to the aversion to fructose-containing foods, remarkable absence of dental caries was noted. • The defect resides in aldolase B, which catalyzes the cleavage of fructose-1-phosphate to form dihydroxyacetone phosphate and D-glyceraldehyde.
Phenotype • Hypoglycemia, • Depletion of ATP resources, • Degradation of purine (G and A in DNA), • Hypermagnesemia,
CLINICAL MANAGEMENT • Limit, fructose and related sugars…sucrose and sorbitol, • Difficult, if not impossible in modern, Western society.
Glycolysis • Cells are run by the energy produced through the oxidative conversion of glyceraldehyde 3-phosphate to pyruvate and the coupled formation of ATP and NADH, • You’ve learned the conversion of glucose into G3P, but we can’t live by glucose alone...
Liver, Kidney, Intestinal Mucosa • In aldolase 'B'-deficient tissues, cytoplasmic accumulation of fructose-1-phosphate leads to sequestration of inorganic phosphate with resulting activation of AMP deaminase that catalyzes the irreversible deamination of AMP to IMP (inosine monophosphate), a precursor of uric acid. • Depletion of tissue ATP occurs through massive degradation to uric acid and impairment of regeneration by oxidative phosphorylation in the mitochondria because of inorganic phosphate depletion. • In the cell, ATP exists largely as a 1:1 complex with magnesium. Depletion of ATP in tissues leads to depletion also of magnesium concentration.
AKA: aldolase B Feeder Pathways for Glycolysis
Lactose intolerance • Lactose Intolerance is divided into the following categories: • 1. Congenital Alactasia or hypolactasia This is an extremely rare condition except in Scandinavian countries. Babies with this condition do not gain weight and are dehydrated and extremely unwell. • 2. Primary acquired or lactase non-persistence. This is an age related condition and usually occurs after weaning and before the age of six years. This affects approximately 70% of the world’s population and 10% of Australia’s population overall. • 3. Secondary acquired or lactase non-persistence occurs as a result of damage to the small intestinal mucosa due to for example gastroenteritis, cows milk protein intolerance or coeliac disease. OMIM#: 223000
Polymorphic • A149Pand A174D frequencies near 1%, • no obvious advantage has been identified for heterozygotes, although physiological manifestestions of heterozygosity exist, • Overall frequency in the population of homozygotes is between 1 in 15,000 to 1 in 20,000.
Aldolase B Mutations • > 21 mutations that have been reported; • 15 of these are single-base substitutions, • resulting in 9 amino acid replacements, • 4 nonsense codons, • and 2 putative splicing defects. • The other 6 were deletions. • Recurrent mutations were observed in exons 5 and 9. Analysis suggests that the A149Pand A174D mutations originated from a single founder and achieved a relatively high frequency through genetic drift.
Mutant Alleles • .0001 FRUCTOSE INTOLERANCE [ALDOB, ALA149PRO] • A G-to-C transversion in exon 5 resulted in a substitution of proline for alanine at position 149 of the protein within a region critical for substrate binding. • .0002 FRUCTOSE INTOLERANCE [ALDOB, ALA174ASP] • Point mutation found in Italy, Switzerland, and Yugoslavia but not in the UK, France, or the United States. • .0003 FRUCTOSE INTOLERANCE [ALDOB, LEU288DEL] • A 1-bp deletion in codon 288 causing a frameshift. The mutation seems restricted to Sicilian subjects. • 0006 FRUCTOSE INTOLERANCE [ALDOB, ASN334LYS] • In addition, in 11 unrelated Italian patients, researchers found a G-to-C transversion in exon 9 which resulted in substitution of lysine for asparagine at position 334. • .0008 FRUCTOSE INTOLERANCE [ALDOB, ARG3TER] • A consanguineous family from eastern Turkey, has a C-to-T transition in codon 3 changing arg to stop codon. • .0011 FRUCTOSE INTOLERANCE [ALDOB, LEU182DEL, VAL183DEL ] • In a 6-year-old patient with a 6-bp deletion in exon 6 of the aldolase B gene that led to elimination of 2 amino acid residues, leu182 and val183, but left the message in-frame. On the other allele, the patient carried the asn334-to-lys mutation.
Structure/Mutation Sites • Aldolase B associates in quartenary structure as a homotetramer, • A149P and A147D mutations result in a reduced affinity between sub-units. • Other mutation my retain quatenary structure, but lack enzymatic activity.
OMIM http://www.ncbi.nlm.nih.gov:80/entrez/dispomim.cgi?id=229600
Sickling and G6PD Defenciencies • Heterozygotes carrying alleles for for red blood cell sickling disorders, and for and glucose-6-phosphate dehydrogenase deficiency are resistant to malaria.
Sickle Cell Anemia • Walter Clement Noel, a first-year dental student at the Chicago College of Dental Surgery, was admitted to the Presbyterian Hospital in late 1904 where Ernest E. Irons, a 27-year-old intern, obtained a history and performed routine physical, blood, and urine examinations. • He noticed that Noel's blood smear contained 'many pear-shaped and elongated forms' and alerted his attending physician, James B. Herrick, to the unusual blood findings.
Sickling Disease in Modern Culture • Homozygotes for sickling disorders have from mild ranging to debilitating disorders, • Heterozygotes and homozygotes have health complications in temperate climates due to cold temperatures, and endemic infections.
G6PD Disease in Modern Culture • First seen in WWII, African-American soldiers receiving an anti-malaria drug experienced haemolysis. • Presently, • Sulphanomides, • Anti-pyretic drugs, • Broad Beans.
MWF (1-2 pm), Autumn Quarter, Literature driven course, Genomics, Sequencing. Reverse genetics, DNA Arrays, etc. Transcriptomics, DNA arrays, EST library analysis, etc. Proteomics, Protein Chips, 2-D gels, Mass Spectroscopy, Metabolomics, Phenomics, Who-knows-what-omics. Learn how to read and understand cutting edge papers, Low-key environment. Functional Genomics(445)
"I guess there's cool stuff about science," Watanabe continued, "like space travel and bombs. But that stuff is so hard, it's honestly not even worth the effort."
IMPORTANT INSTRUCTIONS FOR ADMINISTERING COURSE EVALUATIONS PLEASE FOLLOW EXACTLY! 1. INSTRUCTOR: Tell students who will administer the evaluation, and advise them whether they are dismissed afterward. Then please read the following two statements to the class exactly as written, and LEAVE THE ROOM DURING THE EVALUATION : "I have scheduled time today for you to rate the quality of this course. The University and I take the evaluation of teaching very seriously and hope you will approach this evaluation thoughtfully. The results of this evaluation will help to improve the course in the future, and also may influence decisions concerning tenure, promotion, or salary. Your participation is voluntary and confidential; to ensure confidentiality, do not write your name on the forms. There is a possibility your handwriting on the written comment sheet might be recognizable; however, I will not see the results of this evaluation until after the quarter is over and you have received your grades." "Please be sure to use a NO.2 PENCIL ONLY to fill in ovals on the evaluation form."