Download
1 / 30
310 likes | 469 Views
Prospective Study Cohort Study Assis.Prof.Dr Diaa Marzouk Community Medicine. What is a cohort?. A cohort is a group of persons who share a common experience within a defined time period. Healthy cohorts are followed up forward in time for the development of a disease. Examples of cohorts:.

E N D
Prospective Study Cohort Study Assis.Prof.Dr Diaa MarzoukCommunity Medicine
What is a cohort? A cohort is a group of persons who share a common experience within a defined time period. Healthy cohorts are followed up forward in time for the development of a disease
Examples of cohorts: Birth cohort: All persons born within a given period of time. Marriage cohort: All persons married within a given period of time Occupational cohort:
Selection of cohorts: Volunteers: Because it is acssesable From armed forces: Because its medical records are available Have particular exposue: At work
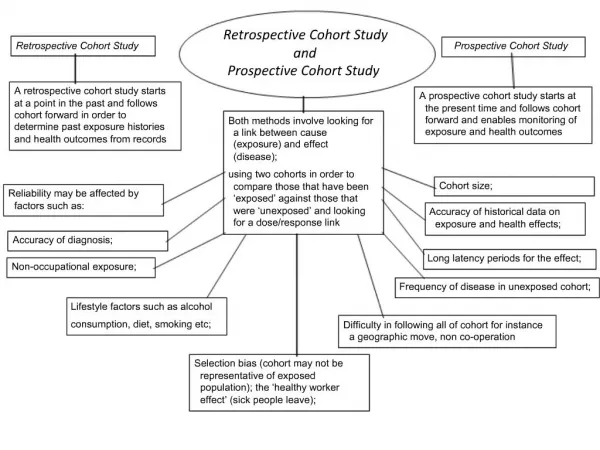
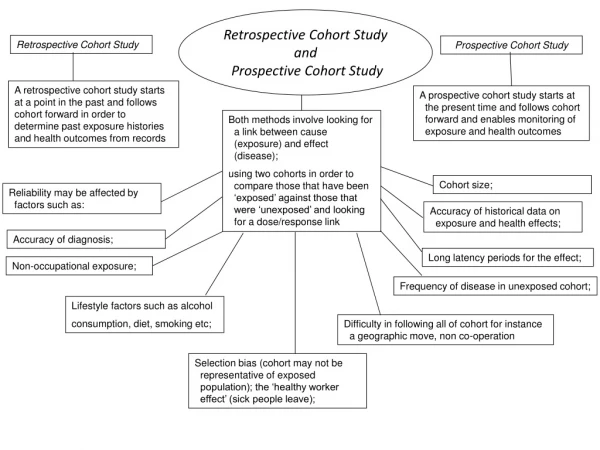
Prospective StudyCohort Study It starts with a group of people / cohort: All considered to be free of a given disease. But vary in exposure to a supposed risk factor.
Information is gathered about their exposure to the suspected risk factor The individuals are divided into exposed and not exposed To the factor of interest
The cohort is followed over time in order to determine differences in the rate at which disease develops in relation to exposure to the factor
Retrospective StudiesCase Control St. Diseased and nondiseased groups (cases and controls) are selected and compared for presence or absence of antecedent factor (risk factor)
Advantages of Prospective Study The cohort is classified in relation to exposure to the factor before the disease develops This classification cannot be influenced by the knowledge that disease exists.
2. It permits calculation of Incidence rates among exposed and not exposed. 3. Theabsolute difference between both is the attributable risk. 3. The relative risk.
4. Permits observation of many outcomes, e.g smoking and lung cancer, showed that smoking is associated with other otcomes as emphysema, CHD, peptic ulcer, cancer larynx, oral cavity, oesopphagus and urinary bladder.
Disadvantages of Prospective studies Long, expensive and large scale undertaking. The problem of attrition: loss of patients due to lack of interest, migration or death from other causes.
3. Changes in diagnostic criteria and methods over time 4. Administrative problems as loss of staff, loss of funding, and the high costs of record keeping
Analysis of Results Anlytic studies are designed to determine whether an association exsists between a factor or exposure and a disease and to determine the strength of the association.
Relative Risk It is an important measure of association that relates the incidence rates of the disease under study among those with and without the factor or exposure.
Relative Risk It is defined as the ratio of the incidence rate for persons exposed to the incidence rate for those not exposed.
Relative Risk (RR)= Incidence among exposed Incidence among unexposed
Diseased Not Diseased Exposed a b Not Exposed c d RR= a ÷ c = ad a+b c+d bc
Historical Prospective Studies It combines the advantages of both retrospective and prospective study desgins. It involves following healthy exposed and unexposed cohorts for the development of the disease.
These cohorts are constructed retrospectively through existing records that permit correct classification of the exposure status of individuals
Study subjectd are traced to the present time or sometimes to the future as well. The analysis of this study is as the prospective study.
Examples of Cohort Studies I- OBJECTIVE:To identify risk factors for breast cancer among female survivors of childhood cancer. Exposure: Survivors of childhood cancer are at risk for secondary breast cancer. DESIGN:Retrospective cohort study. SETTING:The Childhood Cancer Survivor Study (CCSS), a multicenter study of persons who survived more than 5 years after childhood cancer diagnosed from 1970 to 1986.
PARTICIPANTS: Among 6068 women in the CCSS, 95 women had 111 confirmed cases of breast cancer. MEASUREMENTS: Standardized incidence ratios for breast cancer were calculated by using age-specific incidence rates in the general population. Breast cancer incidence was evaluated with respect to primary cancer diagnosis and therapy, age at and time since primary diagnosis, menstrual and reproductive history, and family history of cancer.
RESULTS: Breast cancer risk was increased in survivors who were treated with chest radiation therapy (standardized incidence ratio, 24.7 [95% CI, 19.3 to 31.0]) and survivors of bone and soft-tissue sarcoma who were not treated with chest radiation therapy (standardized incidence ratios, 6.7 and 7.6, respectively).
CONCLUSION: Survivors of childhood sarcomas and those who received chest radiation therapy are at risk for secondary breast cancer. When assessing a survivor's risk, clinicians should consider primary diagnosis, previous radiation therapy, family cancer history, and history of thyroid disease.
II-Growth in prepubertal children with cystic fibrosis In cystic fibrosis, growth and lung function have been identified as prognostic markers of both severity of pulmonary disease and survival. Objective: longitudinal design to determine whether normalisation of growth could be found in the genetic subgroup of prepubertal children with CFwith the homozygous Delta F508 mutation, which is one of the known severe mutations.
METHODS: Data of all children born after 1980 with the homozygous Delta F508 mutation, diagnosed in early childhood at the specialised centre of the Children's Hospital of Berne were systematically assessed up to the age of 11 years and retrospectively analysed. Follow-up data of height, weight and BMI were compared to the Swiss reference population using z-scores.
RESULTS: In the study, cohort growth (height, weight and BMI) was significantly below that of the normal Swiss population. A significant decline of lung function with age was also found, however, no association between lung function and growth could be seen. Compared to an earlier cohort, an improved growth over the last decade could be shown but no improvement on lung function could be detected
CONCLUSION: In contrast to sequential cross-sectional studies of children with CF, the present longitudinal study of children with homozygous for the Delta F508 mutation failed to confirm normalisation of growth over time.