Download
1 / 27
270 likes | 478 Views
PRESENTED BY : MARIAM TARIQ ROLL # 144 AND MARIA SYED ROLL # 140. Clinical features and morphology of myocarditis : . Lymphocytic myocarditis as a cause of fulminant heart failure (scenario) :.

E N D
PRESENTED BY : MARIAM TARIQ ROLL # 144 AND MARIA SYED ROLL # 140 Clinical features and morphology of myocarditis :
Lymphocyticmyocarditis as a cause of fulminant heart failure (scenario) : • A 63-year-old woman with prior systemic hypertension was well until 39 days before death when she fainted in her kitchen and was hospitalized. An electrocardiogram and telemetry monitoring disclosed : • sinus bradycardia(50 beats per minute) with • first-degree atrioventricular block, • left bundle branch block, • An echocardiogram showed mitral regurgitation and an ejection fraction of 60%. • An angiogram disclosed normal coronary arteries. The left ventricular and aortic pressures were normal.
During her 3 days in the hospital, she had recurrent sinus pauses with associated syncope, • and a permanent atrioventricular sequential pacemaker was implanted. • Thereafter, she felt well and was active • Then it was until 22 days before she died, whenexertional dyspnea appeared and progressed, prompting rehospitalization 20 days before death. • Her blood pressure was 120/75 mm Hg, • her paced heart rate was 80 beats per minute, • and her temperature was normal • Decreased breath sounds at both lung bases. • A chest radiograph showed pulmonary vascular congestion, cardiomegaly, and bilateral pulmory effusions.
Over the subsequent 19 days in the hospital, the patient's status progressively deteriorated • She also developed hemodynamically unstable atrial fibrillation and had multiple electrical cardioversions. • At necropsy, • the heart weighed 470 grams. • The quantity of subepicardialadipose tissue was increased. • The coronary arteries were widely patent with no identifiable plaques. • All 4 cardiac chambers were dilated (Figure). • The 4 valves were anatomically normal. • Multiple myocardial lesions were present grossly in the left ventricular wall and ventricular septum, • and histologically numerous foci of lymphocytic infiltrates were present with associated myocardial cell necrosis and foci of replacement fibrosis (Figure)
The heart in the patient described. • View of dilated right and left ventricles just caudal to the atrioventricular valves. • Transverse cuts of the cardiac ventricles. • Close-up view of the ventricular septum and right and left ventricular walls.
This patient had a clinical course of about 40 days, and it was characterized initially by syncope. • Her final 20 days were characterized by progressive and finally fatal heart failure. Cardiac studies during her final days disclosed angiographicallynormal coronary arteries but generalized inadequate cardiac function. • This short clinical course suggests, of course, an acute myocarditis that would be characterized by • the presence of numerous polymorphonuclear leukocytes in the myocardial walls, • histologically, however, was seen the presence of numerous lymphocytes in the ventricular walls and associated microventricular scars compatible with her 40-day course.
CLINICAL FEATURES : • The signs and symptoms of myocarditis vary, depending on the cause and the severity of the disease. The most common signs and symptoms include: • Chest pain that may feel like a heart attack or angina • A rapid or abnormal heartbeat (arrhythmia) • Shortness of breath, at rest or during physical activity • Fluid retention with swelling of legs, ankles and feet • Fatigue • Fever is present in 20% of patients.
Less-common signs and symptoms include: • Fainting or a sudden loss of consciousness • Other symptoms may be with a viral infection, such as a headache, body aches, joint pain, fever, a sore throat or diarrhea • Sometimes, people with myocarditis will also develop pericarditis, which is an inflammation of the membrane covering the heart (pericardium). Pericarditis may cause sharp pains over the center of chest.
MILD MYOCARDITIS : • In mild cases, myocarditis may have no noticeable symptoms, • may feel ill , • have general symptoms of a viral infection , • never realize that heart is affected. • Some people may never seek medical care and may recover without ever knowing they had myocarditis.
Myocarditis in children : • When children develop myocarditis, they may experience these signs and symptoms: • Fever • Loss of appetite • Breathing difficulties • Bluish or grayish discoloration of the skin
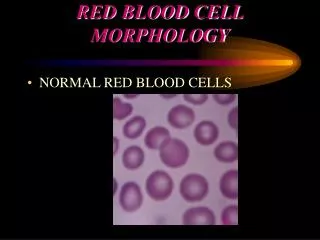
MYOCARDITIS : The picture at far left shows the opened heart with some very dark red areas visible on the left side (see arrow). The picture at near left is a dissected strip of heart muscle. The large dark areas are the areas of infection. The bottom image is a photomicrograph of the heart muscle. The lower half of the photomicrograph shows normal heart muscle cells. The upper half of the picture shows how the muscle fibers have been destroyed by the infection.
In this case, a young man was found dead on his bed when he was called for supper. • There were needle marks in his arm and enlarged lymph nodes at the base of his liver. • He had developed myocarditis( an infection of the heart muscle) from using dirty needles. • After a significant amount of heart muscle was destroyed, the young man died.
Morphology and Microbiologic features: • Gross evaluationof the heart reveals : • flabby and pale muscle with petechiae. • Ventricular muscle is usually thinand may be hypertrophied. • Heart valves and the endocardium are not usually involved
Morphology and Microbiologic features • Myocarditis is most frequently induced by cardio tropic viruses including coxsackievirus, echovirus and influenza virus as well as parvovirus and herpes virus. This leads to: • focal destructionof cardiac muscle cells, • interstitial myocardial fibrosisfollowing • vascular exudation as an interstitial edema, and later to • polymorphonuclear and round cellinfiltrationbetween the muscle fibers, • as well as macrophagessurrounding necrotic cardiomyocytes.
Morphology and Microbiologic features (brief theoratical description of various types): • Acuteisolated myocarditis: a frequently fatal, idiopathic, acute myocarditis affecting chiefly the interstitial fibrous tissue. • Fiedler's myocarditis : acute isolated myocarditis • Giantcell myocarditis: a subtype of acute isolated myocarditis characterized by the presence of multinucleate giant cells and other inflammatory cells, and by ventricular dilatation, mural thrombi, and wide areas of necrosis.
Morphology and Microbiologic features • Granulomatous myocarditis : • giant cell myocarditis, including also granuloma formation. • Hypersensitivity myocarditis : • due to allergic reactions caused by hypersensitivity to various agents, particularly sulfonamides, penicillins , and methyldopa. • Interstitial myocarditis : • affecting chiefly the interstitial fibrous tissue.
The microscopic hallmark of acute myocarditis is: • Focal or diffuse interstitial infiltrate of mononuclear cells, lymphocytes, plasma cells, and eosinophils. • Viral particles are rarely seen unless searched with special techniques (ie, PCR). • Necrosis and disarrangement of the myocytes are typical and often are seen with coxsackievirus infection. • In the chronic and healing stages, myocytes are replaced by fibroblasts (scar tissue). • In adenoviral myocarditis, less severe infiltrate can be seen histologically than is seen in cases of enteroviral infection.
Histologic Findings : • Acute myocarditis • Histopathological image of acute myocarditis at autopsy in a patient withacute onset of congestive heart failure
2. Adenoviral (AV) myocarditis in a young adult man (37 years old). Adenoviral (AV) myocarditis in a young adult man (37 years old). (a) Histology of EMB showing lymphomonocyte inflammatory cell infiltrates associated with myocyte injury. No viral inclusion bodies are evident. Hematoxylin and eosin × 100. (b) PCR analysis for adenovirus: lane 1: DNA marker; lane 2: AV positive control; lane 3: EMB AV PCR positive; lane 4: beta-globin (house-keeping gene); lane 5: negative control (reagents without template).
3. HYPERSENSITIVITY MYOCARDITIS . Hypersensitivity myocarditis : High magnification of myocardium with perivascular infiltrates rich in eosinophils. This patient had a clinical history compatible with drug-induced hypersensitivity myocarditis.
4. Giant Cell Myocarditis: Giant cell myocarditis (GCM) is a rare inflammatory disease of the myocardium that often affects previously healthy young adults.
Gross:Gross appearance of the heart is not unlike that seen in myocarditis associated with known infectious agents, “ the essential features being dilatation and sometimes hypertrophy”. When the lesions are extensive, they appear as yellow-gray or gray foci throughout the myocardium. Mural thrombi are commonly present. Microscopic features:After common causes of heart disease are excluded, the diagnosis must be confirmed by endomyocardial biopsy. Histologic findings, of widespread or multifocalserpiginousnecrosis with mixed inflammatory infiltrate composedof lymphocytes and histiocytes are considered diagnostic. Thepresence of eosinophils is noted in most cases. Admixed withthe infiltrate are multinucleated giant cells. The giant cells are of the Foreign body and Langhans types, but some giant cells of myogenic origin also may be present.
Echocardiographic findings in fulminant and acute myocarditis : Echocardiographic findings in patients with fulminant and acute myocarditis at baseline and six months. (A) Fractional shortening, (B) left ventricular end-diastolic dimension, (C) septal thickness. ∗p < 0.01 vs. acute; †p < 0.01 for interaction between time and type of myocarditis.
Endomyocardialbiopsy specimens from patients with fulminant (A) and acute (B) myocarditis. Fulminant myocarditis was characterized by more extensive and diffuse lympocytic infiltration and myocyte necrosis than acute myocarditis. (hematoxylin-eosin stain, original magnification × 400).