Download
1 / 1
10 likes | 157 Views
Post Transplantation Lymphoproliferative Disorder After Intestinal Transplantation. Vrakas G, Reddy S, Collins G, Friend PJ, Vaidya A. Oxford Transplant Centre, Oxford OX3 7NR, UK. RESULTS. INTRODUCTION. METHODS.

E N D
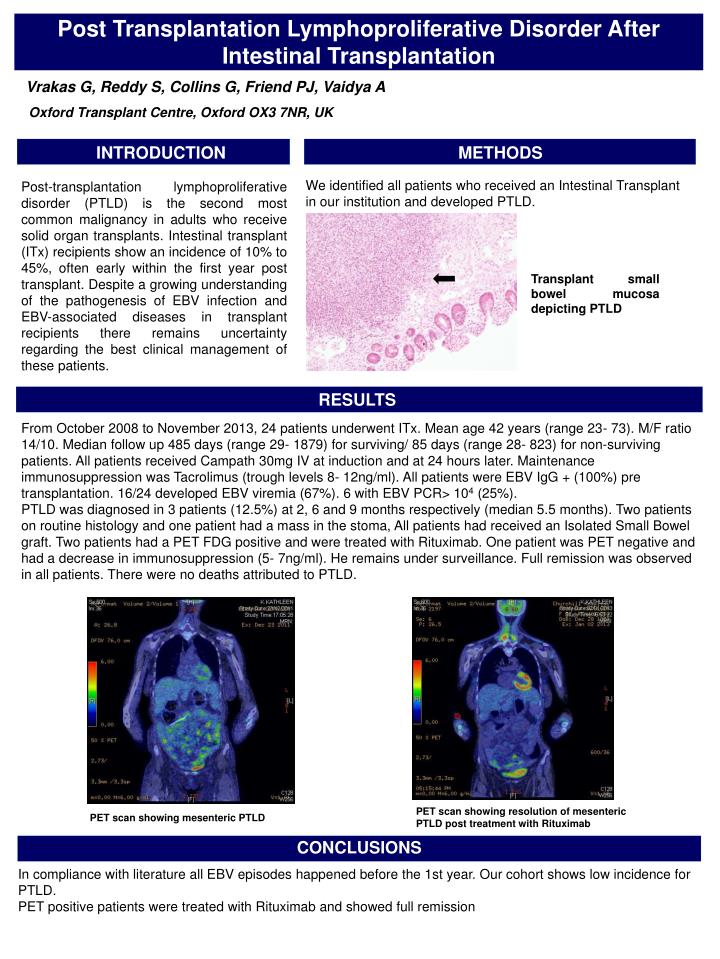
Post Transplantation Lymphoproliferative Disorder After Intestinal Transplantation Vrakas G, Reddy S, Collins G, Friend PJ, Vaidya A Oxford Transplant Centre, Oxford OX3 7NR, UK RESULTS INTRODUCTION METHODS We identified all patients who received an Intestinal Transplant in our institution and developed PTLD. Post-transplantation lymphoproliferative disorder (PTLD) is the second most common malignancy in adults who receive solid organ transplants. Intestinal transplant (ITx) recipients show an incidence of 10% to 45%, often early within the first year post transplant. Despite a growing understanding of the pathogenesis of EBV infection and EBV-associated diseases in transplant recipients there remains uncertainty regarding the best clinical management of these patients. Transplant small bowel mucosa depicting PTLD From October 2008 to November 2013, 24 patients underwent ITx. Mean age 42 years (range 23- 73). M/F ratio 14/10. Median follow up 485 days (range 29- 1879) for surviving/ 85 days (range 28- 823) for non-surviving patients. All patients received Campath 30mg IV at induction and at 24 hours later. Maintenance immunosuppression was Tacrolimus (trough levels 8- 12ng/ml). All patients were EBV IgG + (100%) pre transplantation. 16/24 developed EBV viremia (67%). 6 with EBV PCR> 104 (25%). PTLD was diagnosed in 3 patients (12.5%) at 2, 6 and 9 months respectively (median 5.5 months). Two patients on routine histology and one patient had a mass in the stoma, All patients had received an Isolated Small Bowel graft. Two patients had a PET FDG positive and were treated with Rituximab. One patient was PET negative and had a decrease in immunosuppression (5- 7ng/ml). He remains under surveillance. Full remission was observed in all patients. There were no deaths attributed to PTLD. PET scan showing resolution of mesenteric PTLD post treatment with Rituximab PET scan showing mesenteric PTLD CONCLUSIONS In compliance with literature all EBV episodes happened before the 1st year. Our cohort shows low incidence for PTLD.PET positive patients were treated with Rituximab and showed full remission


![-A g [X g ]](https://cdn3.slideserve.com/5611649/a-g-x-g-dt.jpg)