Download
1 / 40
410 likes | 495 Views
Learn about American College of Physicians' current goals, challenges in healthcare, and the High-Value, Cost-Conscious Care Initiative. Find out how ACP is promoting excellence in medicine and advocating for better patient care.

E N D
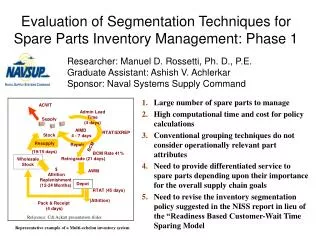
What is the ACP Doing These Days? Fred Ralston, Jr. MD FACP President American College of Physicians 2011 Nevada Chapter Scientific Meeting Saturday, January 15, 2011 Las Vegas, Nevada
ACP Goals • I. To establish and promote the highest clinical standards and ethical ideals; • II. To be the foremost comprehensive education and information resource for all internists; • III. To advocate responsible positions on individual health and on public policy relating to health care for the benefit of the public, our patients, the medical profession, and our members;
ACP Goals • IV. To serve the professional needs of the membership, support healthy lives for physicians, and advance internal medicine as a career; • V. To promote and conduct research to enhance the quality of practice, the education and continuing education of internists, and the attractiveness of internal medicine to physicians and the public.
ACP Goals • VI. To recognize excellence and distinguished contributions to internal medicine; and • VII. To unify the many voices of internal medicine and its subspecialties for the benefit of our patients, our members, and our profession.
Lofty goals How are we doing? • For patients? • For those who pay the bills? • To provide proper incentives to encourage good behavior? • For internists?
Who can we look to in order to improve health care? • Government – Congress and the Executive Branch • Patients • Business community • Insurers • Professional organizations including ACP • Who best can change health care expections and individual lifestyle choices?
What do we know? • We have evidence that enhanced primary care is associated with lower costs and better outcomes • We see increasing evidence that The Patient-Centered Medical Home (PCMH) Model increases satisfaction among patients, health care workers and lowers costs • That the current payment and delivery model is unsustainable
Primary care physicians are paid less. • A primary care physician could earn $3 million less over a career than a cardiologist – a disparity that significantly influences the career choices of medical students. Vaughn, et al. Can We Close The Income And Wealth Gap Between Specialists and Primary Care, Health Affairs, May, 2010, http://content.healthaffairs.org/cgi/content/abstract/29/5/933 • To achieve the desired ratio of practicing primary care physicians, the average incomes of these physicians must achieve at least 70% of median incomes of all other physicians. Council on Graduate Medical Education, 20th Annual Report, May 2010
What shouldn’t the government do? • Demand that primary care practices accept excessive financial risk. • Fail to deliver on the promise to reduce time involved in health plan interactions. (Remember HIPAA?) • Impose even more regulatory burdens and excessive reporting requirements. • Evaluate models only on their ability to control costs.
What shouldn’t the government do? • Detract from movement to create truly collaborative teams by advocating for APNs as substitutes for primary care physicians. • Try to force all primary care into large groups. • Create models that only work for large groups. • Require too much regulation and not enough innovation. • Undermine private sector and state innovation.
Imaging • Great advances in order to help our patients • Large component of rise in cost of medical care • Huge “hassle factor” in prior approval • Studies begat studies in generating follow-up of incidental findings • Imaging should be ordered and reimbursed as appropriate adjunct to medical care -- not to subsidize “loss leader” of E&M services
Imaging in an ideal world • Guidelines in various clinical situations agreed upon and made easily available to practicing physicians and patients • Imaging following these guidelines easy to obtain • Process to deal with overutilization, particularly when owned by the physician or practice
ACP High-Value, Cost-Conscious Care Initiative Physicians and patients need evidence-based information so they can make the right decision about the right treatment at the right time. High-value, cost-conscious care is about eliminating overused and misused medical treatments that do not improve patient health or might even be harmful.
ACP High-Value, Cost-Conscious Care Initiative The initiative will include the development of ACP’s High-Value, Cost-Conscious Care Recommendations by ACP’s Clinical Efficacy Assessment Technical Advisory Committee that will be submitted for review and consideration for publication in Annals of Internal Medicine. The effort will address common medical conditions for which inappropriate use of resources is known to be an issue such as low back pain.
Patient-Centered Medical Home • Advances primary care through payment and delivery reforms • Good for all specialties in that it provides an anchor where the patient goes for first contact care and where care is coordinated for a variety of conditions • Allows for subspecialty relationship as “medical neighbor” or medical home for certain conditions
Patient-Centered Medical Home • Needs adequate financing to provide initial capital for information systems, connectivity, training, practice transformation and adequate staff support • Needs adequate financing to pay primary doctors and other team members competitive salaries to attract appropriate talent
Patient-Centered Medical Home • Provides the potential for data collection and reporting as a single seamless continuous quality improvement process • With that data collection allows the opportunity to test various models of care • Initial data indicates patient, staff and physician satisfaction along with cost savings
What are our options? • Current “system” is not sustainable – costs will bankrupt us • We need to align incentives to encourage the outcomes we desire • We need to test and continuously improve delivery of primary care and the PCMH appears to be the best option to do this
Changing What Patients Look For • Old goal: Best Heart Surgery in the Region • New goal: Those we care for now have the lowest incidence of heart disease in the region – but if you do develop heart disease we have the best heart surgery and procedures in the region
Changing How Patients Behave Old asks: • Isn’t there a pill for that? • Can’t I just get an MRI so I will know? • What specialist do I need to see for this? • Can you talk at Rotary about your hospital’s newest machine or procedure?
Changing How Patients Behave New asks: • How much exercise should I be doing? • I saw a drug ad on TV – what’s really going on? • What’s the most cost-effective way to manage my condition? • Can you come talk at Rotary about lifestyle choices and prevention?
Most importantly • Having a place to ask those questions • Having a doctor who has the time and resources to recommend the best treatment for your overall health • Having the resources to connect you with others when he/she can’t provide that care • Having the cost of the care affordable for us as individuals and as a society
ACP Activities • Advocate for laws, administrative interpretation and implementation that advance our goals • Work on administrative simplification to reduce or eliminate many hassle factors • Provide or direct members to resources that assist in practice transformation
Ways of Explaining “The Health Bill” • Short version: Search Cokie Roberts Kaiser Family Foundation Health Report 9 Minute Cartoon on uTube Does an Excellent Job Explaining Key Points • Listen to Bob Doherty outline it from the perspective of the ACP DC Office
Challenge for ACP • Help members and public understand that with or without the ACA, rising costs are the single greatest challenge facing the health care system, and the status quo is not an option. • Let’s lead a national discussion of how to control costs while achieving the best outcomes.
Work Ahead for ACP • Influence design and implementation of ACOs, PCMHs, bundling, and CER. • Propose own ideas for controlling costs while improving quality and oppose cost controls that are not in members’ or patients’ interests. • Advocate for more meaningful liability reforms.
Culture • Rather than looking to Washington, the answer may lie in a “culture” in our own communities • "Health-care costs ultimately arise from the accumulation of individual decisions doctors make about which services and treatments to write an order for” • The “battle for the soul of American medicine” is over “whether the doctor is set up to meet the needs of the patient, first and foremost, or to maximize revenue.” Gawande: The Cost Conudrum, What a Texas Town Can Teach Us About Health Care, Atlantic Monthly, June 1, 2009, http://www.newyorker.com/reporting/2009/06/01/090601fa_fact_gawande?currentPage=article
Culture:But how do you explain Provo? • “If there is any place that should have medical spending under control, this is it. Residents of Provo, many of them Mormons who don't smoke or drink, are among the healthiest in the country... Until recently, Provo seemed to be a model for the nation. But spending on Medicare patients here has accelerated rapidly. . . The culprit: a swift increase in the number of procedures and tests being performed - a trend that has coincided with the additions of new surgical and cancer treatment suites and diagnostic machines at hospitals and clinics throughout the growing region.” Washington Post, Increase in health tests, procedures is raising costs in frugal Utah, May 18, 2010, http://www.washingtonpost.com/wp-dyn/content/article/2010/05/17/AR2010051703822.html
What this means for ACP: • We need to lead a discussion on how to change a culture of over-use, without assigning “blame.” • Issues to be considered: medical education and training, physician self-referral, ethical and professional responsibility to be responsible stewards, development and implementation of appropriateness guidelines, shared medical decision-making and patient responsibility.
What this means for ACP • Influence development of new models to give patients and physicians the principal responsibility for control of the money, but with accountability for results. • May result in confrontation with other stakeholders. • Help members successfully participate in new models—especially smaller practices.
Help from ACP: • ACP position papers are available at www.acponline.org • ACP Advocate newsletter. • ACP Advocate blog with Bob Doherty, http://advocacyblog.acponline.org/ • Follow Bob on Twitter @BobDohertyACP
Help from ACP • Need help selecting an EHR? • AmericanEHR Partners program, http://www.americanehr.com/Home.aspx • Want to learn more about the PCMH? Visit ACP’s PCMH resource center: • http://www.acponline.org/running_practice/pcmh/ • Want to assess your own readiness to become a PCMH? • Medical Home Builder, http://www.acponline.org/running_practice/pcmh/help.htm
Back to Basics • ACP is hard at work to advance our goals for the benefit of the public, our patients, the medical profession, and our members; • The Educational Resources of ACP are continuously improved and available now in a variety of formats
ACP Foundation • Great Work on Health Literacy http://www.acpfoundation.org/health_lit.htm • Health Tips http://www.acpfoundation.org/hl/htips.htm
ACP International • New Chapter established in Saudi Arabia • Interest in a Chapter in India • FACP is a mark of excellence recognized throughout the world • With the internet ACP Educational Resources are readily available throughout the world to advance medical knowledge and practice
What is the ACP Doing These Days? • 130,000 Members Strong in an era with less joiners • Tremendous resources available from talented staff • Volunteer efforts of many leaders and huge pool of talent since members rarely say no when asked to do something for “The College”
ACP Goals • I. To establish and promote the highest clinical standards and ethical ideals; • II. To be the foremost comprehensive education and information resource for all internists; • III. To advocate responsible positions on individual health and on public policy relating to health care for the benefit of the public, our patients, the medical profession, and our members;
ACP Goals • IV. To serve the professional needs of the membership, support healthy lives for physicians, and advance internal medicine as a career; • V. To promote and conduct research to enhance the quality of practice, the education and continuing education of internists, and the attractiveness of internal medicine to physicians and the public.
ACP Goals • VI. To recognize excellence and distinguished contributions to internal medicine; and • VII. To unify the many voices of internal medicine and its subspecialties for the benefit of our patients, our members, and our profession.
Questions or comments? Fred Ralston, Jr. MD FACP Private Practice General Internal Medicine Fayetteville Medical Associates 207 South Elk Avenue Fayetteville, Tennessee 37334 ralston@fpunet.com President American College of Physicians