Download
1 / 1
10 likes | 257 Views
ABSTRACT

E N D
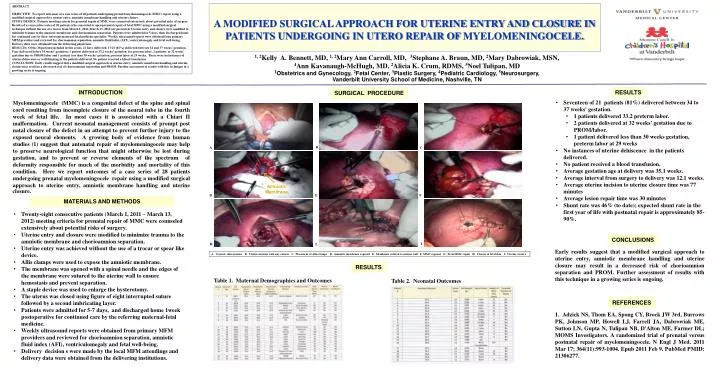
ABSTRACT OBJECTIVE: To report outcomes of a case series of 28 patients undergoing prenatal myelomeningocele (MMC) repair using a modified surgical approach to uterine entry, amniotic membrane handling and uterine closure.STUDY DESIGN: Patients meeting criteria for prenatal repair of MMC were counseled extensively about potential risks of surgery. Results of a consecutive series of 28 patients who consented to open prenatal repair of fetal MMC using a modified surgical technique without the use of a trocar from March 1, 2011-March 13, 2012 are presented. Uterine entry and closure were modified to minimize trauma to the amniotic membrane and chorioamnion separation. Patients were admitted for 5 days, then discharged home for continued care by their referring maternal-fetal medicine specialist. Weekly ultrasound reports were obtained from primary MFM providers and reviewed for chorioamnion separation, amniotic fluid index (AFI), ventriculomegaly and fetal well-being. Delivery data were obtained from the delivering physicians.RESULTS: Of the 28 patients included in this series, 21 have delivered. 17/21 (81%) delivered between 34 and 37 weeks’ gestation. Four delivered before 34 weeks’ gestation: 1 patient delivered at 33.2 weeks’ gestation for preterm labor, 2 patients at 32 weeks’ gestation due to PROM/labor and 1 patient less than 30 weeks’ gestation, preterm labor at 29 weeks. There were no instances of uterine dehiscence or wall thinning in the patients delivered. No patient received a blood transfusion.CONCLUSION: Early results suggest that a modified surgical approach to uterine entry, amniotic membrane handling and uterine closure may result in a decreased risk of chorioamnion separation and PROM. Further assessment of results with this technique in a growing series is ongoing. A MODIFIED SURGICAL APPROACH FOR UTERINE ENTRY AND CLOSURE IN PATIENTS UNDERGOING IN UTERO REPAIR OF MYELOMENINGOCELE. 1, 2Kelly A. Bennett, MD, 1, 2Mary Ann Carroll, MD, 3Stephane A. Braun, MD, 2Mary Dabrowiak, MSN, 4Ann Kavanaugh-McHugh, MD, 2Alicia K. Crum, RDMS, 5Noel Tulipan, MD 1Obstetrics and Gynecology, 2Fetal Center, 3Plastic Surgery, 4Pediatric Cardiology, 5Neurosurgery, Vanderbilt University School of Medicine, Nashville, TN RESULTS INTRODUCTION SURGICAL PROCEDURE Myelomeningocele (MMC) is a congenital defect of the spine and spinal cord resulting from incomplete closure of the neural tube in the fourth week of fetal life. In most cases it is associated with a Chiari II malformation. Current neonatal management consists of prompt post natal closure of the defect in an attempt to prevent further injury to the exposed neural elements. A growing body of evidence from human studies (1) suggest that antenatal repair of myelomeningocele may help to preserve neurological function that might otherwise be lost during gestation, and to prevent or reverse elements of the spectrum of deformity responsible for much of the morbidity and mortality of this condition. Here we report outcomes of a case series of 28 patients undergoing prenatal myelomeningocele repair using a modified surgical approach to uterine entry, amniotic membrane handling and uterine • Seventeen of 21 patients (81%) delivered between 34 to 37 weeks' gestation. • 1 patients delivered 33.2 preterm labor. • 2 patients delivered at 32 weeks’ gestation due to PROM/labor. • 1 patient delivered less than 30 weeks gestation, preterm labor at 29 weeks • No instances of uterine dehiscence in the patients delivered. • No patient received a blood transfusion. • Average gestation age at delivery was 35.1 weeks. • Average interval from surgery to delivery was 12.1 weeks. • Average uterine incision to uterine closure time was 77 minutes • Average lesion repair time was 30 minutes • Shunt rate was 46% (to date); expected shunt rate in the first year of life with postnatal repair is approximately 85- 90%. A C D F B A C closure. MATERIALS AND METHODS I G • Twenty-eight consecutive patients (March 1, 2011 – March 13, 2012) meeting criteria for prenatal repair of MMC were counseled extensively about potential risks of surgery. • Uterine entry and closure were modified to minimize trauma to the amniotic membrane and chorioamnion separation. • Uterine entry was achieved without the use of a trocar or spear like device. • Allis clamps were used to expose the amniotic membrane. • The membrane was opened with a spinal needle and the edges of the membrane were sutured to the uterine wall to ensure hemostasis and prevent separation. • A staple device was used to enlarge the hysterotomy. • The uterus was closed using figure of eight interrupted suture followed by a second imbricating layer. • Patients were admitted for 5-7 days, and discharged home 1week postoperative for continued care by the referring maternal-fetal medicine. • Weekly ultrasound reports were obtained from primary MFM providers and reviewed for chorioamnion separation, amniotic fluid index (AFI), ventriculomegaly and fetal well-being. • Delivery decision s were made by the local MFM attendings and delivery data were obtained from the delivering institutions. Amniotic Membrane CONCLUSIONS F D E Early results suggest that a modified surgical approach to uterine entry, amniotic membrane handling and uterine closure may result in a decreased risk of chorioamnion separation and PROM. Further assessment of results with this technique in a growing series is ongoing. A. Vertical skin incision B. Uterine incision with stay sutures C. Placement of Allis clamps D. Amniotic membrane exposed E. Membrane sutured to uterine wall FMMC exposed G. Fetal MMC repair H. Closure of fetal skin I. Uterine closure RESULTS Table 1. Maternal Demographics and Outcomes Table 2. Neonatal Outcomes REFERENCES I H I 1. Adzick NS, Thom EA, Spong CY, Brock JW 3rd, Burrows PK, Johnson MP, Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB, D'Alton ME, Farmer DL; MOMS Investigators. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011 Mar 17; 364(11):993-1004. Epub 2011 Feb 9. PubMed PMID: 21306277.