Download
1 / 1
10 likes | 162 Views
Pharmacists’ Interventions to Decrease Child Obesity at a Community Hospital Laura Erhardt, Pharm. D Candidate, Stacie Thoman, Pharm. D Candidate Kristin K. Johnson, B.S., Pharm. D., BCPS Abby A. Kahaleh, B.S. Pharm., MPH., PhD. Lake Erie College of Osteopathic Medicine School of Pharmacy .

E N D
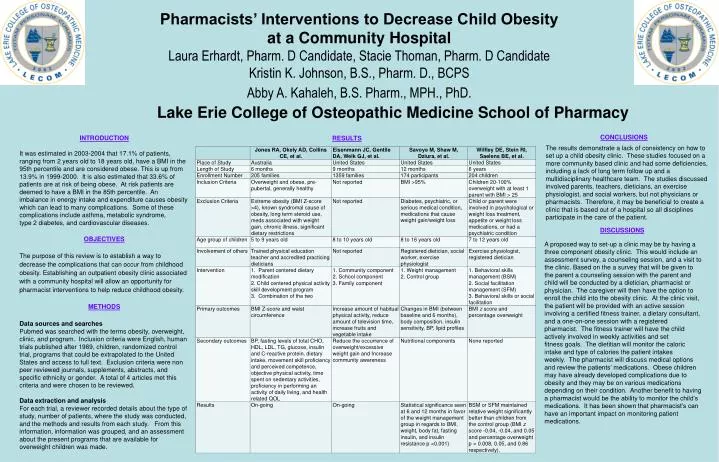
Pharmacists’ Interventions to Decrease Child Obesity at a Community Hospital Laura Erhardt, Pharm. D Candidate, Stacie Thoman, Pharm. D Candidate Kristin K. Johnson, B.S., Pharm. D., BCPS Abby A. Kahaleh, B.S. Pharm., MPH., PhD. Lake Erie College of Osteopathic Medicine School of Pharmacy INTRODUCTION It was estimated in 2003-2004 that 17.1% of patients, ranging from 2 years old to 18 years old, have a BMI in the 95th percentile and are considered obese. This is up from 13.9% in 1999-2000. It is also estimated that 33.6% of patients are at risk of being obese. At risk patients are deemed to have a BMI in the 85th percentile. An imbalance in energy intake and expenditure causes obesity which can lead to many complications. Some of these complications include asthma, metabolic syndrome, type 2 diabetes, and cardiovascular diseases. OBJECTIVES The purpose of this review is to establish a way to decrease the complications that can occur from childhood obesity. Establishing an outpatient obesity clinic associated with a community hospital will allow an opportunity for pharmacist interventions to help reduce childhood obesity. METHODS Data sources and searches Pubmed was searched with the terms obesity, overweight, clinic, and program. Inclusion criteria were English, human trials published after 1989, children, randomized control trial, programs that could be extrapolated to the United States and access to full text. Exclusion criteria were non peer reviewed journals, supplements, abstracts, and specific ethnicity or gender. A total of 4 articles met this criteria and were chosen to be reviewed. Data extraction and analysis For each trial, a reviewer recorded details about the type of study, number of patients, where the study was conducted, and the methods and results from each study. From this information, information was grouped, and an assessment about the present programs that are available for overweight children was made. CONCLUSIONS RESULTS The results demonstrate a lack of consistency on how to set up a child obesity clinic. These studies focused on a more community based clinic and had some deficiencies, including a lack of long term follow up and a multidisciplinary healthcare team. The studies discussed involved parents, teachers, dieticians, an exercise physiologist, and social workers, but not physicians or pharmacists. Therefore, it may be beneficial to create a clinic that is based out of a hospital so all disciplines participate in the care of the patient. DISCUSSIONS A proposed way to set-up a clinic may be by having a three component obesity clinic. This would include an assessment survey, a counseling session, and a visit to the clinic. Based on the a survey that will be given to the parent a counseling session with the parent and child will be conducted by a dietician, pharmacist or physician. The caregiver will then have the option to enroll the child into the obesity clinic. At the clinic visit, the patient will be provided with an active session involving a certified fitness trainer, a dietary consultant, and a one-on-one session with a registered pharmacist. The fitness trainer will have the child actively involved in weekly activities and set fitness goals. The dietitian will monitor the caloric intake and type of calories the patient intakes weekly. The pharmacist will discuss medical options and review the patients’ medications. Obese children may have already developed complications due to obesity and they may be on various medications depending on their condition. Another benefit to having a pharmacist would be the ability to monitor the child’s medications. It has been shown that pharmacist’s can have an important impact on monitoring patient medications.