Download
1 / 1
20 likes | 116 Views
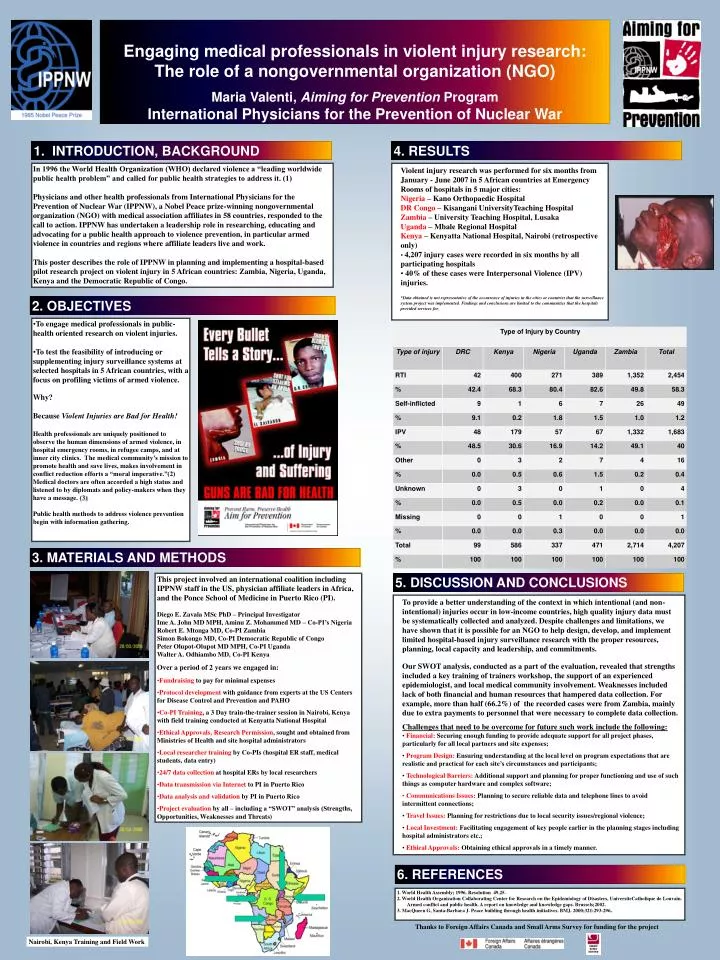
LOGO. Engaging medical professionals in violent injury research: The role of a nongovernmental organization (NGO) Maria Valenti, Aiming for Prevention Program International Physicians for the Prevention of Nuclear War. LOGO. 1. INTRODUCTION, BACKGROUND. 4. RESULTS.

E N D
LOGO Engaging medical professionals in violent injury research: The role of a nongovernmental organization (NGO) Maria Valenti, Aiming for Prevention ProgramInternational Physicians for the Prevention of Nuclear War LOGO 1. INTRODUCTION, BACKGROUND 4. RESULTS In 1996 the World Health Organization (WHO) declared violence a “leading worldwide public health problem” and called for public health strategies to address it. (1) Physicians and other health professionals from International Physicians for the Prevention of Nuclear War (IPPNW), a Nobel Peace prize-winning nongovernmental organization (NGO) with medical association affiliates in 58 countries, responded to the call to action. IPPNW has undertaken a leadership role in researching, educating and advocating for a public health approach to violence prevention, in particular armed violence in countries and regions where affiliate leaders live and work. This poster describes the role of IPPNW in planning and implementing a hospital-based pilot research project on violent injury in 5 African countries: Zambia, Nigeria, Uganda, Kenya and the Democratic Republic of Congo. • Violent injury research was performed for six months from January - June 2007 in 5 African countries at Emergency Rooms of hospitals in 5 major cities: • Nigeria – Kano Orthopaedic Hospital • DR Congo – Kisangani UniversityTeaching Hospital • Zambia – University Teaching Hospital, Lusaka • Uganda – Mbale Regional Hospital • Kenya – Kenyatta National Hospital, Nairobi (retrospective only) • 4,207 injury cases were recorded in six months by all participating hospitals • 40% of these cases were Interpersonal Violence (IPV) injuries. • *Data obtained is not representative of the occurrence of injuries in the cities or countries that the surveillance system project was implemented. Findings and conclusions are limited to the communities that the hospitals provided services for. 2. OBJECTIVES • To engage medical professionals in public-health oriented research on violent injuries. • To test the feasibility of introducing or supplementing injury surveillance systems at selected hospitals in 5 African countries, with a focus on profiling victims of armed violence. • Why? • Because Violent Injuries are Bad for Health! • Health professionals are uniquely positioned to observe the human dimensions of armed violence, in hospital emergency rooms, in refugee camps, and at inner city clinics. The medical community’s mission to promote health and save lives, makes involvement in conflict reduction efforts a “moral imperative.”(2) Medical doctors are often accorded a high status and listened to by diplomats and policy-makers when they have a message. (3) • Public health methods to address violence prevention begin with information gathering. 3. MATERIALS AND METHODS • This project involved an international coalition including IPPNW staff in the US, physician affiliate leaders in Africa, and the Ponce School of Medicine in Puerto Rico (PI). • Diego E. Zavala MSc PhD – Principal Investigator • Ime A. John MD MPH, Aminu Z. Mohammed MD – Co-PI’s Nigeria • Robert E. Mtonga MD, Co-PI Zambia • Simon Bokongo MD, Co-PI Democratic Republic of Congo • Peter Olupot-Olupot MD MPH, Co-PI Uganda • Walter A. Odhiambo MD, Co-PI Kenya • Over a period of 2 years we engaged in: • Fundraising to pay for minimal expenses • Protocol development with guidance from experts at the US Centers for Disease Control and Prevention and PAHO • Co-PI Training, a 3 Day train-the-trainer session in Nairobi, Kenya with field training conducted at Kenyatta National Hospital • Ethical Approvals, Research Permission, sought and obtained from Ministries of Health and site hospital administrators • Local researcher training by Co-PIs (hospital ER staff, medical students, data entry) • 24/7 data collection at hospital ERs by local researchers • Data transmission via Internet to PI in Puerto Rico • Data analysis and validation by PI in Puerto Rico • Project evaluation by all – including a “SWOT” analysis (Strengths, Opportunities, Weaknesses and Threats) 5. DISCUSSION AND CONCLUSIONS • To provide a better understanding of the context in which intentional (and non-intentional) injuries occur in low-income countries, high quality injury data must be systematically collected and analyzed. Despite challenges and limitations, we have shown that it is possible for an NGO to help design, develop, and implement limited hospital-based injury surveillance research with the proper resources, planning, local capacity and leadership, and commitments. • Our SWOT analysis, conducted as a part of the evaluation, revealed that strengths included a key training of trainers workshop, the support of an experienced epidemiologist, and local medical community involvement. Weaknesses included lack of both financial and human resources that hampered data collection. For example,more than half (66.2%) of the recorded cases were from Zambia, mainly due to extra payments to personnel that were necessary to complete data collection. • Challenges that need to be overcome for future such work include the following: • Financial: Securing enough funding to provide adequate support for all project phases, particularly for all local partners and site expenses; • Program Design: Ensuring understanding at the local level on program expectations that are realistic and practical for each site’s circumstances and participants; • Technological Barriers: Additional support and planning for proper functioning and use of such things as computer hardware and complex software; • Communications Issues: Planning to secure reliable data and telephone lines to avoid intermittent connections; • Travel Issues: Planning for restrictions due to local security issues/regional violence; • Local Investment: Facilitating engagement of key people earlier in the planning stages including hospital administrators etc.; • Ethical Approvals: Obtaining ethical approvals in a timely manner. 6. REFERENCES 1. World Health Assembly; 1996. Resolution 49.25. 2. World Health Organization Collaborating Center for Research on the Epidemiology of Disasters, UniversiteCatholique de Louvain. Armed conflict and public health. A report on knowledge and knowledge gaps. Brussels;2002. 3. MacQueen G, Santa-Barbara J. Peace building through health initiatives. BMJ. 2000;321:293-296. Thanks to Foreign Affairs Canada and Small Arms Survey for funding for the project Nairobi, Kenya Training and Field Work


![Engaging Undergraduates in Research [and Inquiry]](https://cdn1.slideserve.com/2053051/engaging-undergraduates-in-research-and-inquiry-dt.jpg)