Download
1 / 22
220 likes | 396 Views
In-house vs. Out-sourced Clinical Engineering. David M. Dickey, CHC, CCE Corporate Director, McLaren Health Care Clinical Engineering Services. Disclaimer/Transparency. I do have a biased opinion! 30+ years managing in-house clinical engineering programs

E N D
In-house vs. Out-sourced Clinical Engineering David M. Dickey, CHC, CCE Corporate Director, McLaren Health Care Clinical Engineering Services
Disclaimer/Transparency • I do have a biased opinion! • 30+ years managing in-house clinical engineering programs • Currently Corporate Director CE McLaren Health Care • 15+ years clinical engineering consulting (Medical Technology Management., Inc.) www.mtminc.org • Practice area focus is in creating and/or expansion of CE programs • Conversion of out-sourced programs to in-house • Having been in this profession for my entire career, I know a lot of CE professionals that have ‘gone both ways’, switching back and forth as needed
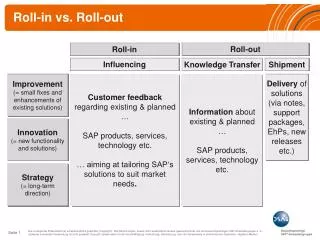
I do agree • Out-sourced programs may make sense for smaller hospitals, < 100-150 beds, especially if they are not part of a larger system with internal CE resources • Not all in-house, or out-sourced, programs are created equal • Common factors that impact degree of success • Quality and education of the staff • Resources • Administrative support • ‘Fix it’ shop vs. a ‘professional service’…what are the needs? • Either type of program is doomed for failure if the program delivered does not fit the needs and expectations of the organization! • Neither are free
Example of cash impact if you outsource • If inventory is $290,000,000 • COSR = 4.7% Budget is then $13,630,000 • Outsource to a provide that has 20% profit margin, cost now becomes $16,356,000 (COSR now 5.6%) • If hospital’s net annual operating margin is 2%, the additional $’s paid needs to be made up by the hospital collection of 100% on $13,630,000 of patient charges!
Issues of concern when converting to in-house from out-sourced program • Software CMMS and data conversions • Test equipment and tools • Manuals • Over due PMs and CM’s wip credits • Staffing and ability to hire providers staff • Contracts and OEM discounts • Policies and procedures • Clerical and call center support • Clinical engineering expertise • Three to six months lead time
In order to convert to an in-house model • Develop a business plan (three years), based on cost and quality • Set realistic goals and expectations • Consolidate all service budgets into one • Include contract/vendor management services • Start with general biomedical equipment support • Plan for expansion into service of ultrasound; sterilization; imaging; cath lab; clinical lab; radiation oncology; surgical instrument mgt.
If you have an out-sourced program • Perform bi-annual assessment of equipment actually serviced, PM or CM, and remove from inventory items never seen, to lower your program contract cost • Read your contract and verify deliverables are being delivered • Negotiate the margin, full disclosure of all costs • If vendor gets credits for parts returned, it should be credited back to the hospital • Mandate full staffing levels. If not met, get credit • Mandate credits for PM’s not done on time • Obtain quarterly downloads (Excel format) of inventory and work histories • Consider getting help…call me when you are ready to save money! (daved@mtminc.org)