Download
1 / 86
880 likes | 1.24k Views
Refraction. Light rays are bent refractive index = ratio of light in a vacuum to the velocity in that substance velocity of light in vacuum=300,000 km/sec Light year 9.46 X 10 12 km Refractive indices of various media air = 1 cornea = 1.38 aqueous humor = 1.33 lens = 1.4

E N D
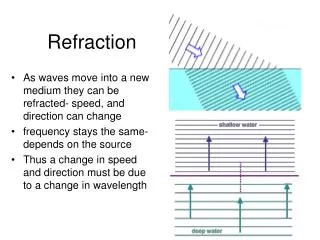
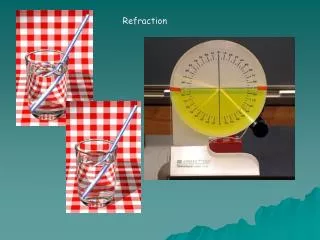
Refraction • Light rays are bent • refractive index = ratio of light in a vacuum to the velocity in that substance • velocity of light in vacuum=300,000 km/sec • Light year 9.46 X 1012 km • Refractive indices of various media • air = 1 • cornea = 1.38 • aqueous humor = 1.33 • lens = 1.4 • vitrous humor = 1.34
Refraction of light by the eye • Refractive power of 59 D (cornea & lens) • Diopter = 1 meter/ focal length • Convex lens expressed as + diopters • Concave lens expressed as - diopters • central point 17 mm in front of retina • inverted image- brain makes the flip • lens strength can vary from 20- 34 D (Δ 14) • Ability to increase refractive power ⇓ with age • 14 (age 10) 8 (age 30) 2 (age 50) • Parasympathetic + increases lens strength • Greater refractive power needed to read text
Accomodation • Increasing lens strength from 20 -34 D • Parasympathetic + causes contraction of ciliary muscle allowing relaxation of suspensory ligaments attached radially around lens, which becomes more convex, increasing refractive power (illustration) • Associated with close vision (e.g. reading) • In addition, eyes roll in and pupils constrict • Presbyopia- loss of elasticity of lens w/ age • decreases accommodation
Errors of Refraction • Emmetropia- normal vision; ciliary muscle relaxed in distant vision • Hyperopia-“farsighted”- focal pt behind retina • globe short or lens weak ; convex lens to correct • Myopia- “nearsighted”- focal pt in front of retina • globe long or lens strong’; concave lens to correct • Astigmatism- irregularly shaped • cornea (more common) • lens (less common)
Visual Acuity • Snellen eye chart • ratio of what that person can see compared to a person with normal vision • 20/20 is normal • 20/40 less visual acuity • What the subject sees at 20 feet, the normal person could see at 40 feet. • 20/10 better than normal visual acuity • What the subject sees at 20 feet, the normal person could see at 10 feet
Visual acuity • The fovea centralis is the area of greatest visual acuity • it is less than .5 mm in diameter (< 2 deg of visual field) • outside fovea visual acuity decreases to more than 10 fold near periphery • acuity for point sources of light 25 sec of arc (angle of 25 seconds) • point sources of light two apart on retina can be distinguished as two separate points
Fovea and acute visual acuity • Central fovea-area of greatest acuity • composed almost entirely of long slender cones • aids in detection of detail • blood vessels, ganglion cells, inner nuclear & plexiform layers are displaced laterally • allows light to pass relatively unimpeded to receptors
Depth Perception • Relative size • the closer the object, the larger it appears • learned from previous experience • Moving parallax • As the head moves, objects closer move across the visual field at a greater rate • Stereopsis- binocular vision • eyes separated by 2 inches- slight difference in position of visual image on both retinas, closer objects are more laterally placed
Formation of Aqueous Humor • Secreted by ciliary body (epithelium) • 2-3 ul/min • flows into anterior chamber and drained by Canal of Schlemm (vein) • intraocular pressure- 12-20 mmHg. • Glaucoma- increased intraocular P. • compression of optic N.-can lead to blindness • treatment; drugs & surgery
Retina • Peripheral extension of the CNS • Processing of visual signal • Photoreceptors • Rods & Cones • Other Cells • bipolar, ganglion, horizontal, amacrine • Only retinal cells that generate action potentials are the ganglion cells
Photoreceptors • Rods & Cones • Light breaks down rhodopsin (rods) and cone pigments (cones) • rhodopsin Na+ conductance • photoreceptors hyperpolarize • release less NT (glutamate) when stimulated by light
Dark Rod/Cone depolarize ↑ NT Hyperpol Depolarize “ON” BC “OFF BC Light Rod/Cone hyperpolarize NT Depolarize Hyperpol “ON” BC “OFF” BC Retinal responses
Bipolar Cells • Connect photoreceptors to either ganglion cells or amacrine cells • passive spread of summated postsynaptic potentials (No AP) • Two types • “ON”- hyperpolarized by NT glutamate • Invaginating bipolars • “OFF”- depolarized by NT glutamate • Flat bipolars
Ganglion Cells • Can be of the “ON” or “OFF” variety • “ON” bipolar + “ON” ganglion • “OFF” bipolar + “OFF” ganglion • Generate AP carried by optic nerve • Three subtypes • X (P) cells • Y (M) cells • W cells
P (X) Ganglion Cells • Most numerous (55%) G cells • Receive input mostly from bipolar c. • Slower conduction velocity (14 m/sec) • Sustained response-slow adaptation • Small receptive field • signals represent discrete retinal location • Respond differently to different • Responsible for color vision • Project to Parvocellular layer of lateral geniculate nucleus (thalamic relay)
M (Y) Ganglion Cells • Receive input mostly from Amacrine • Larger receptive field • Transient-fast conduction velocity • respond best to moving stimuli • Not sensitive to different • More sensitive to brightness • Project to magnocellular LGN • Black & White images
W Ganglion Cells • smallest, slowest CV (8 m/sec) • 40% of all ganglion cells • many lack center-surround antagonistic fields • they act as light intensity detectors • some respond to large field motion • detect directional movement • Broad receptive fields • Receive most of their input from rods • Important for crude vision in dim light
Horizontal Cells • Non spiking inhibitory interneurons • Make complex synaptic connections with photorecetors • Hyperpolarized when light stimulates input photoreceptors (just like receptor) • When they depolarize they inhibit photoreceptors • Maybe responsible for center-surround antagonism
Amacrine Cells • Receive input from bipolar cells • Project to ganglion cells • Several types releasing different NT • GABA, dopamine • Transform sustained “ON” or “OFF” to transient depolarization & AP in ganglion cells
Center-Surround Fields • Receptive fields of bipolar & gang. C. • two concentric regions • Center field • mediated by all photoreceptors synapsing directly onto the bipolar cell • Surround field • mediated by photoreceptors which gain indirect access to bipolar cells via horizontal cells
Center-Surround (cont) • Photoreceptors contributing to center field of one bipolar cell contributes to surround field of other bipolar cells • Because of center-surround antagonism, ganglion cells monitor differences in luminance between center & surround fields
Center-surround (cont) • If center field is on, surround is off • If center field is off, surround is on • Simultaneous stimulation of light of both fields gives no net response • antagonistic excitatory & inhibitory inputs neutralize each other • When surround is illuminated, the horizontal cells depolarize the cones in the center (opposite effect of light)
Receptive field size • In fovea- ratio can be as low as 1 cone to 1 bipolar cell to 1 ganglion cell • In peripheral retina- hundreds of rods can supply a single bipolar cell & many bipolar cells connected to 1 ganglion cell
Dark Adaptation • In sustained darkness reformation of light sensitive pigments (Rhodopsin & Cone Pigments) • of retinal sensitivity 10,000 fold • cone adaptation<100 fold (1st 10 min.) • rod adaptation>100 fold (50 min.) • dilation of pupil • neural adaptation
Cones • 3 populations of cones with different pigments-each having a different peak absorption • Blue sensitive (445 nm) • Green sensitive (535 nm) • Red sensitive (570 nm)
Color Blindness • Sex-linked trait carried on X chromosome • Occurs almost exclusively in males but transmitted by the female • Most common is red-green color blindness • missing either red or green cones
Loss of Cones • Loss of Red Cones- Protanope • decrease in overall visual spectrum • Loss of Green Cones- Deuteranope • normal overall visual spectrum • problems distinguishing green, yellow, orange & red (Ishihara Chart) • Loss of Blue Cones- rare but may be under-represented “Blue weakness”
Visual Pathway • Optic N to Optic Chiasm • Optic Chiasm to Optic Tract • Optic Tract to Lateral Geniculate • Lateral Geniculate to 10 Visual Cortex • geniculocalcarine radiation
Additional Visual Pathways • From Optic Tracts to: • Suprachiasmatic Nucleus • biologic clock function • Pretectal Nuclei • reflex movement of eyes- • focus on objects of importance • Superior Colliculus • rapid directional movement of both eyes • Orienting reactions
Primary Visual Cortex • Brodman area 17 (V1)-2x neuronal density • Simple Cells-responds to bar of light/dark • above & below layer IV • Complex Cells-motion dependent but same orientation sensitivity as simple cells • Color blobs-rich in cytochrome oxidase in center of each occular dominace band • starting point of cortical color processing • Vertical Columns-input into layer IV • Hypercolumn-functional unit, block through all cortical layers about 1mm2
Visual Association Cortex • Visual signal is broken down & sent over parallel pathways • Visual analysis proceeds along many paths in parallel- at least 30 cortical areas processing vision • Parvo-interblob • High resolution static form perception (B & W) • Blob • Color (V4) • Achromatopsia • Magno • Movement (MT) & Stereoscopic Depth
Old vs. New visual system • Old pathway projects to the superior colliculus • Locating objects in visual field, so you can orient to it (rotate head & eyes) • Subconscious • Blindsight • New pathway projects to the cortex • Consciously recognizing objects
Blindsight • Some patients who are effectively blind because of brain damage can carry out tasks which appear to be impossible unless they can see the objects. • For instance they can reach out and grasp an object, accurately describe whether a stick is vertical or horizontal, or post a letter through a narrow slot. • The explanation appears to be that visual information travels along two pathways in the brain. If the cortical pathway is damaged, a patient may lose the ability to consciously see an object but still be aware of its location and orientation via projections to the superior colliculus at a subconscious level. • How the brain learns to see video
Cortical fixation areas • Voluntary fixation mechanism (anterior) • Person moves eyes voluntarily to fix on an object • Controlled by cortical field bilaterally in premotor cortex • Involuntary fixation mechanism (posterior) • Holds eyes firmly on object once it has be located • Controlled by secondary visual areas in occipital cortex located just in front of primary visual cortex • Works in conjunction with the superior colliculus • Involuntary fixation is mostly lost when superior colliculus is destroyed.
Control of Pupillary Diameter • Para + causes size of pupil (miosis) • Symp + causes size of pupil (mydriasis) • Pupillary light reflex • optic nerve to pretectal nuclei to Edinger-Westphal to ciliary ganglion to pupillary sphincter to cause constriction (Para)
Horner’s Syndrome • Interruption of SNS supply to an eye • from cervical sympathetic chain • constricted pupil compared to unaffected eye • drooping of eyelid normally held open in part by SNS innervated smooth muscle • dilated blood vessels • lack of sweating on that side of face
Function of extraoccular muscles • Medial rectus of one eye works with the lateral rectus of the other eye as a yoked pair to produce lateral eye movements • The superior& inferior recti muscles elevate & depress the eye respectively and are most effective when the eye is abducted • The superior oblique muscles lower the eye when it is adducted • The inferior oblique muscle elevates the eye when it is adducted
Innervation of extraoccular muscles • Extraoccular muscles controlled by CN III, IV, and VI • CN VI controls the lateral rectus only • CN IV controls the superior oblique only • CN III controls the rest
Sound • Units of Sound is the decibel (dB) • I (measured sound) • Decibel = 1/10 log -------------------------- • I (standard sound) • Reference Pressure for standard sound • .02 X 10-2 dynes/cm2
Sound • Energy is proportional to the square of pressure • A 10 fold increase in sound energy = 1 bel • One dB represents an actual increase in sound E of about 1.26 X • Ears can barely detect a change of 1 dB
Different Levels of Sound • 20 dB- whisper • 60 dB- normal conversation • 100 dB- symphony • 130 dB- threshold of discomfort • 160 dB- threshold of pain
Frequencies of Audible Sound • In a young adult • 20-20,000 Hz (decreases with age) • Greatest acuity • 1000-4000 Hz
Tympanic Membrane & Ossicles • Impedance matching-between sound waves in air & sound vibrations generated in the cochlear fluid • 50-75% perfect for sound freq.300-3000 Hz • Ossicular system • reduces amplitude by 1/4 • increases pressure against oval window 22X • increased force (1.3) • decreased area from TM to oval window (17)
Ossicular system (cont.) • Non functional ossicles or ossicles absent • decrease in loudness about 15-20 dB • medium voice now sounds like a whisper • attenuation of sound by contraction of • Stapedius muscle-pulls stapes outward • Tensor tympani-pull malleous inward
Attenuation of sound • CNS reflex causes contraction of stapedius and tensor tympani muscles • activated by loud sound and also by speech • latency of about 40-80 msec • creation of rigid ossicular system which reduces ossicular conduction • most effective at frequencies of < 1000 Hz. • Protects cochlea from very loud noises, masks low freq sounds in loud environment
Cochlea • System of 3 coiled tubes • Scala vestibuli • Scala media • Scala tympani