Download
1 / 43
430 likes | 528 Views
Culture and Context: Lessons from a Sub-Saharan African Experience. Rachel Hingst, OTR, CPRP. Learning Objectives:. Attendees will be able to: Describe cultural values which are reflected in the principles and practice of psychiatric rehabilitation in the United States

E N D
Culture and Context: Lessons from a Sub-Saharan African Experience Rachel Hingst, OTR, CPRP
Learning Objectives: Attendees will be able to: Describe cultural values which are reflected in the principles and practice of psychiatric rehabilitation in the United States Explain some of the specific challenges faced by both individuals with mental illness and service providers in developing countries Recognize their responsibility as global citizens to advocate for mental health to be prioritized on the international health agenda
Session Outline: Introduction to Sub-Saharan Africa American cultural values, norms, and assumptions Small group work Presentations of group work Challenges Examples of practices Questions/discussion
“Developing countries” Developing/developed Least Developed Countries (LDC) Less Economically Developed Country (LEDC) Non-industrialized/industrialized Third world/first world Global south/global north Majority World
If the world was a village... If the world's population was reduced to 100 people: 60 Asians, 14 Africans, 12 Europeans, 8 Latin Americans, 5 from the USA and Canada, and 1 from the South Pacific 67 would be unable to read 50 would be malnourished and 1 dying of starvation 24 would not have any electricity (And of the 76 that do have electricity, most would only use it for light at night.) 1 would have a college education 5 would control 32% of the entire world's wealth; all 5 would be US citizens 33 would be receiving --and attempting to live on-- only 3% of the income of "the village"
Global Mental Health: WHO estimates 450 million people worldwide experience mental health problems: 154 million: depression 25 million: schizophrenia 91 million: alcohol use disorders Spending in developing countries: Most middle and low-income countries devote less than 1% of their health expenditure to mental health.
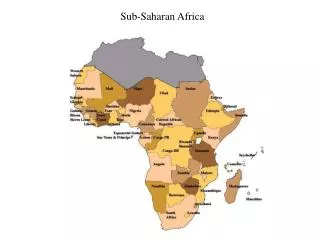
Sub-Saharan Africa: What words come to mind?
Sub-saharan Africa Population of over 800 million Diversity: 1000 different languages Shared experiences
Resources: Ivory and slaves Copper, cotton, rubber, diamonds, tea, tin Oil, gold, platinum, uranium, coltan
The Scramble for Africa: End of 19th century Colonization: artificial boundaries Minority governments Apartheid
Independence: Decolonization Some challenges with independence: human resource and infrastructure...
Politics: Dictatorships One-party states
Economics: Average GDP per capital in Sub-Saharan Africa: approximately $1,800 (compared to about $46,000 for USA) Almost half of people live on less than $1 a day (extreme poverty)
HIV/AIDS: Accounts for 67% of HIV infections worldwide (about 22 million people) Disrupted communities and families 14 million children are orphans Human resources: loss of productive citizens Stress/grief: psychosocial burden
Psychiatric Rehab? Worked for 2 ½ years in Malawi First in government psychiatric hospital then for NGO providing mental health services Programs included: inpatient hospital, outpatient clinic, community outreach clinics, day rehabilitation program, vocational training school, food security program, street children's program, college for training psychiatric nurses and clinical officers, and programs for children with special needs
Examining American norms, values, and assumptions: “Psychiatric rehabilitation has its origins in a Western humanistic worldview, based predominantly on United States and British culture.”-from USPRA Multicultural Principles
Multicultural Principles: Understanding own culture: “The essence of multiculturalism is the study of one’s own culture and ethnicity as the basis for understanding and identifying with those from others. Interpersonal encounters are not “objective” or “value-free” even when these encounters occur in a therapeutic or rehabilitation relationship.” (from Principle 2) Recognizing Worldview of Others: “Psychiatric rehabilitation practitioners recognize that thought patterns and behaviors are influenced by a person’s worldview, ethnicity and culture of which there are many.” (from Principle 4)
Value: Individual American value: “Rugged individualism” Independence valued over interdependence “...appreciating cultural preferences that value relationships and interdependence, in addition to individuality and independence.” (Principle 7)
Value: Work and Achievement From USPRA Vision: “It promotes a world in which individuals with mental illnesses can recover to achieve successful and satisfying lives in the working, learning and social environments of their choice.”
Value: Work and Achievement Do all cultures highly value work and achievement? “Psychiatric rehabilitation practitioners show respect towards others by accepting cultural values and beliefs that emphasize process or product, as well as harmony or achievement.” (Principle 7) “Most mental health service systems in the U.S. place a great deal of emphasis on outcomes, especially achievement of independence and success in role functioning, such as competitive employment. Psychiatric rehabilitation practitioners recognize that people who use psychiatric rehabilitation services will have a variety of definitions of what constitutes success, satisfaction, and recovery.”
Value: Future Orientation Emphasis on planning and progress: Life goals, short-term and long-term goals, strategic planning, etc. Is this something all cultures can relate to? Importance of the past
Value: Control American dream: we control our own destinies; have the ability to bring prosperity to ourselves Tradition of democracy Automony Not everyone has choices: influenced by political, social, and economic factors Role of fate and the supernatural
Assumption: Infrastructure Roads/transportation Communication: phone, mail, internet Water/sanitation Electricity
Assumption: Healthcare/social service system: Functional structure Human resource Other basic resources: medication, soap, lab tests, etc. Social security/welfare system: housing options, disability benefits, etc.
Assumption: Economic opportunities Employment: diverse economy with various sectors Loans accessible: business, education, housing, etc.
Small Group Work: Each group will be given one principle or practice of psychiatric rehabilitation or a characteristic of recovery-focused services Discuss the challenges and opportunities you anticipate in applying this principle/practice in the context of a developing country Consider the cultural differences, social and political factors, and economic disparities
Challenges in implementing psychiatric rehab services: Based on personal experiences in Malawi In addition to day to day challenges Economic Available support
Traditional Beliefs: Causes of mental illness Witchcraft Traditional healers Locus of control Challenges: adherence to medication/treatment poor; active role in illness management difficult
Stigma Disability in general seen as burden Enormous public stigma Open discrimination by leaders, public figures, and health workers Staff working in mental health also stigmatized Challenges: mental health is relegated to background; no resources allocated; even with good skills clients struggle to have satisfying lives due to public stigma
Donor culture International development sector: controversy Allowances for workshops: “allowance culture”: created by donors Volunteering as a job Donors have the power Challenges: difficult to find committed employees and volunteers; resources spent on trainings with questionable outcomes; Western standards/expectations imposed which may not be needed/realistic/sensible in the context
Evidence Digital divide: how many people in this world have internet access? Imported evidence Validity of tools: cultural bias Capacity for research Outside researchers Challenges: Difficulty measuring outcomes—building an evidence base; relying on imported evidence; alienation of our colleagues across the digital divide
What works? Examples of practices...
Sensitization Employers Police and prison workers Churches Traditional/community leaders Community-level
Relationships with Traditional Healers Early identification of problems Using as part of the team
Skills training Adapting to language and culture Examples: conflict management, problem solving, stress management
Food Security Program “Supported farming” Involves family and community Gives client status/fights stigma Links with housing
Vocational training Various trades for self-employment or community employment Educational support
Business/supported employment “supported employment”--not same as US model Business raises money for service Gives clients work experience Fights stigma
Community-Based Rehabilitation CBR Model for rehabilitation and social integration for people with disabilities See WHO references in handout
Plea for Advocacy: Remember the Majority World Be an advocate for making mental health a global priority “No health without mental health.” Celebrate World Mental Health Day on October 10.