Download
1 / 34
380 likes | 633 Views
October 29, 2008. Session 4: Assessing a Document on Diagnosis. Peter Tarczy-Hornoch MD Head and Professor, Division of BHI Professor, Division of Neonatology Adjunct Professor, Computer Science and Engineering faculty.washington.edu/pth. Using Questionmark Software.

E N D
October 29, 2008 Session 4: Assessing a Document on Diagnosis Peter Tarczy-Hornoch MD Head and Professor, Division of BHI Professor, Division of Neonatology Adjunct Professor, Computer Science and Engineering faculty.washington.edu/pth
Using Questionmark Software • See e-mail “[MIDM] Important - testing your Questionmark login id/web browser before MIDM final exam” for more details • First: get your login id/password from MyGrade • Second: test your login id/password and your computer’s/browser’s ability to save and retrieve you exam: • https://primula.dme.washington.edu/q4/perception.dll • 2 question “Test” exam up until 5P Monday 11/3
Assessing a Document on Diagnosis • Context for Assessing a Diagnosis Document • Diagnosis Statistics • Applying to a Scenario
Diagnostic vs. Therapeutic Studies Diagnostic Testing (What is it?) (Session 4) Patient Data & Information Therapy/Treatment (What do I do for it?) (Session 3) Case specific decision making General Information & Knowledge
Steps to Finding & Assessing Information • Translate your clinical situation into a formal framework for a searchable question (Session 1) • Choose source(s) to search (Session 2) • Search your source(s) (Session 2) • Assess the resulting articles (documents) • Therapy documents (Session 3) • Diagnosis documents (Session 4) • Systematic reviews/comparing documents (Session 5) • Decide if you have enough information to make a decision, repeat 1-4 as needed (ICM, clinical rotations, internship, residency)
Assessing a Document on Diagnosis • Context for Assessing a Diagnosis Document • Diagnosis Statistics • Applying to a Scenario
Many Different Kinds of Tests • Tests predict presence of disease • Types of tests • Screening test: before symptoms appear look for disease • Example: Screening mammograms • Diagnostic test: given symptoms/suggestion of a disease help rule in (confirm) or rule out (reject) a diagnosis • Example: ultrasound of appendix in face of abdominal pain • Gold Standard: a “perfect” test that “definitively” categorizes a patient as having one disease • Example: Surgery to remove appendix and then pathologic exam • Can’t always use Gold Standard => Use diagnostic tests • E.g. high risk/cost, only rules in/out one disease vs. multiple, etc.
The 2x2 Table: Diagnostic Test vs. Gold Standard “Gold Standard Test” “Diagnostic Test” • Non-intuitive labels: • Disease Present = Disease “Positive” (+) = Dz(+) • Test Positive = Test predicting disease present • From patient/provider point of view neither Disease Positive nor Test Positive (+) are good things!
Sensitivity (Sn) “Gold Standard Test” “Diagnostic Test” • Sensitivity is proportion of all people with disease who have a positive test • Sensitivity =TP/(TP+FN) • SnNOut - sensitive test, if negative, rules out disease • Sensitivity useful to pick a test – sensitivity key for screening test
Specificity (Sp) “Gold Standard Test” “Diagnostic Test” • Specificity is proportion of all people without disease who have negative test • Specificity = TN/(FP+TN) • SpPIn – A specific test, if positive, rules in disease • Specificity useful to pick a test – specificity key for diagnostic test
“Cut Off Values” Impact Sn/SpExample: blood sugar to predict diabetes Sensitivity key for screening test Specificity key for diagnostic test
Positive Predictive Value (PPV) “Gold Standard Test” “Diagnostic Test” • PPV is proportion of all people with a positive test who have a disease • PPV=TP/(TP+FP) • PPV is useful to use a test: if you have a positive result for your patient, what % of people with positive results actually have the disease
Negative Predictive Value (NPV) “Gold Standard Test” “Diagnostic Test” • NPV is proportion of all people with a negative test who don’t have a disease • NPV=TN/(FN+TN) • NPV is useful to use a test: if you have a negative result for your patient, what % of people with negative results actually don’t have the disease
Prevalence, pre-test & post-test probabilities • Prevalence: • total cases of disease in the population at given time • 2x2 table: [disease (+)])/[disease (+) + disease (-)] • Pre-test probability: • Estimate of probability/likelihood your patient has a disease before you order your test • Often an estimation based on experience or prevalence • Screening test: pre-test probability = prevalence • Post-test probability: • The probability/likelihood that your patient has a disease, after you get the results of the test back
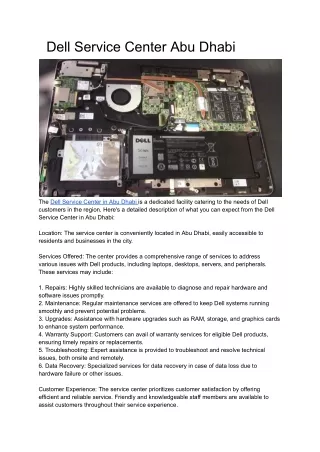
PPV/NPV Dependence on Disease PrevalencePPV Example Sn=TP/(TP+FN)= 450/(450+50)=90% Sp=TN/(FP+TN)= 480/(20+480)=96% PPV=TP/(TP+FP)= 450/(450+20)=95.7% of those with T(+) have Dz(+) Prevalence = 50% Prevalence = 5% Sn=TP/(TP+FN)= 45/(45+5)=90% Sp=TN/(FP+TN)= 912/(912+38)=96% PPV=TP/(TP+FP)= 45/(45+38)=54.2% of those with T(+) have Dz(+) 450 20 45 38 50 480 5 912 Prevalence = 50% Prevalence = 5%
Pros/Cons Sn/Sp/PPV/NPV • Relative Pros: • PPV/NPV useful for diagnosis - probability of disease after (+ ) or (–) test • Sn/Sp useful for choosing a test (screening/diagnosis) • Relative Cons: • PPV/NPV vary with prevalence of disease • Prevalence of disease in general population may not be the same as that of patients you see in clinic/ER • Your estimation of probability of disease (pre-test probability) may not match prevalence in a population • Current tendency therefore => use likelihood ratios Note: Sn/Sp/PPV/NPV on boards
Bayes Theorem • Note: this slide is here for completeness, likelihood ratios better, this slide is thus not on the exam • Bayes Theorem • How to update or revise beliefs in light of new evidence • http://plato.stanford.edu/entries/bayes-theorem/ • Related to Bayes is an alternate form of PPV/NPV as f(Sn, Sp, pre-test) that “pulls out” pre-test probability or prevalence • P(Dz)=probability of disease (e.g. prevalence, pre-test) • PPV=Sn*P(Dz)/[Sn*P(Dz) + (1-Sp)*(1-P(Dz))] • NPV=Sp*(1-P(Dz))/[Sp*(1-P(Dz)) + (1-Sn)*(P(Dz))]
Likelihood Ratios • Likelihood Ratio does NOT vary with prevalence • Likelihood Ratio (LR) • LR+ = Sn/(1-Sp) – likelihood ratio for a positive test • LR- = (1-Sn)/Sp – likelihood ratio for a negative test • Applying LR given a pre-test disease probability: • Pre=Pre-test probability (can be prevalence) • Post=Post-test probability • Post=Pre/(Pre+(1-Pre)/LR) • Same as Bayes & PPV/NPV but cleanly separates test characteristics (LR) from disease prevalence/pre-test probabilities
Interpreting Likelihood Ratios (I) • LR=1.0 • Post-test probability = the pre-test probability (useless) • LR >1.0 • Post-test probability > pre-test probability (helps rule in) • Test result increases the probability of having the disorder • LR <1.0 • Post-test probability < pre-test probability (helps rules out) • Test result decreases the probability of having the disorder • LR+ (Likelihood Ratio for a Positive Test) vs. LR- (Likelihood Ratio for a Negative Test) => See Appendicitis Slide
Interpreting Likelihood Ratios (II) • Likelihood ratios >10 or <0.1 • Test generates large changes in pre- to post-test probability • Test provides strong evidence to rule in/rule out a diagnosis • Likelihood ratios of 5-10 and 0.1-0.2 • Test generates moderate changes in pre- to post-test probability • Test provides moderate evidence to rule in/rule out a diagnosis • Likelihood ratios of 2-5 and 0.2-0.5 • Test generates small changes in pre- to post-test probability • Test provides minimal evidence to rule in/rule out a diagnosis • Likelihood ratios 0.5-2 • Test generates almost no changes in pre- to post-test probability • Test provides almost no evidence to rule in/rule out a diagnosis
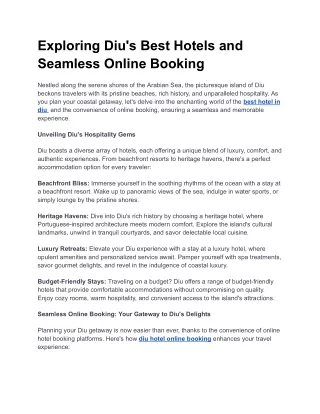
Interpreting Likelihood Ratios (III) • From slide on impact of prevalence: • Sn=90%, Sp=96% • LR+ =0.90/(1-0.96)=22.5 • Post=Pre/(Pre+(1-Pre)/LR) • If prevalence (pre-test) is 50% => post-test 95.7% • If prevalence (pre-test) is 5% => post-test 54.2% LR Nomogram =>
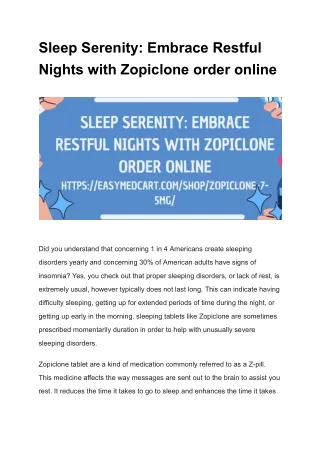
Likelihood Ratios for Physical Exam for Appendicitis Present=“Moderate evidence” for appendicitis Present=“Moderate evidence” for appendicitis BUT 95% CI of LR includes <2 thus includes “Minimal Evidence” LR+ LR- Present=“Almost no evidence” for appendicitis
Assessing a Document on Diagnosis • Context for Assessing a Diagnosis Document • Diagnosis Statistics • Applying to a Scenario
Learning to Diagnose Pneumonia • Medical School • Preclinical: anatomy, histology, pathology, microbiology, pharmacology, physiology,… • Clinical: medicine, pediatrics, family medicine, surgery,…. • Residency: Outpatient, inpatient, specialty rotations, general rotations, emergency room,…. • Fellowship: More of the same • Result: a number of items on history, physical exam, laboratory studies that suggest pneumonia with chest X-ray as gold standard
Literature on Diagnosis of Pneumonia • Clinical query for “pneumonia” “diagnosis” (1478) • Change to “community acquired pneumonia” (181) • Add in “likelihood ratio” (27) • Find “Derivation of a triage algorithm for chest radiography of community-acquired pneumonia patients in the emergency department.” Acad Emerg Med. 2008 Jan;15(1):40-4.
Paper: Background/Objectives • BACKGROUND: Community-acquired pneumonia (CAP) accounts for 1.5 million emergency department (ED) patient visits in the United States each year. • OBJECTIVES: To derive an algorithm for the ED triage setting that facilitates rapid and accurate ordering of chest radiography (CXR) for CAP.
Paper: Methods • METHODS: The authors conducted an ED-based retrospective matched case-control study using 100 radiographic confirmed CAP cases and 100 radiographic confirmed influenzalike illness (ILI) controls. Sensitivities and specificities of characteristics assessed in the triage setting were measured to discriminate CAP from ILI. The authors then used classification tree analysis to derive an algorithm that maximizes sensitivity and specificity for detecting patients with CAP in the ED triage setting.
Paper: Results (I) • RESULTS: Temperature greater than 100.4 degrees F (likelihood ratio = 4.39, 95% confidence interval [CI] = 2.04 to 9.45), heart rate greater than 110 beats/minute (likelihood ratio = 3.59, 95% CI = 1.82 to 7.10), and pulse oximetry less than 96% (likelihood ratio = 2.36, 95% CI = 1.32 to 4.20) were the strongest predictors of CAP. However, no single characteristic was adequately sensitive and specific to accurately discriminate CAP from ILI. • Evidence: • LR>10: Strong, LR 5-10 moderate • 2-5 minimal, 1-2 scant evidence
Paper: Results (II) • RESULTS (continued): A three-step algorithm (using optimum cut points for elevated temperature, tachycardia, and hypoxemia on room air pulse oximetry) was derived that is 70.8% sensitive (95% CI = 60.7% to 79.7%) and 79.1% specific (95% CI = 69.3% to 86.9%). • LR+ =Sn/(1-Sp)=0.708/(1-0.791)=3.39 (minimal) • LR- =(1-Sn)/Sp=(1-0.708)/0.791= 0.37 (minimal) • Post=Pre/(Pre+(1-Pre)/LR) • Post if Pre 1/10 = 0.1/(0.1+(1-0.1))/3.39)=0.27 • Post if Pre 1/2 = 0.5/(0.5+(1-0.5))/3.39)=0.77
Paper: Conclusions • CONCLUSIONS: No single characteristic adequately discriminates CAP from ILI, but a derived clinical algorithm may detect most radiographic confirmed CAP patients in the triage setting. Prospective assessment of this algorithm will be needed to determine its effects on the care of ED patients with suspected pneumonia. • Note: all of these characteristics are among the tried and true findings taught in medical school, residency, fellowship but typically not quantitatively taught
Small Group Monday November 3rd • Students to complete assignment for Small Group Session #5 by Mon 11/3 2-2:50 • Small group leads to give examples of recent clinical situations where they had to evaluate one or more documents related to making a diagnosis • Group to review and discuss from assignment short examples related to diagnosis focusing on: • Sensitivity, Specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) • Likelihood Ratios (Positive/Negative): LR+, LR- • AND/OR: group to search for treatment article(s) on a topic of interest and assess results
QUESTIONS? • Context for Assessing a Diagnosis Document • Diagnosis Statistics • Applying to a Scenario • Small Group Portion