Download
1 / 1
10 likes | 149 Views
Surgical treatment by extra-oral implants in the auricle reconstruction. Chair of Plastic and Reconstructive Surgery – University of Tor Vergata, Rome Italy. Dr Garelli Andrea; Dr Felici Marco ; Dr Masellis Alessandro; Dr Bottini Davide; Dr Galante Vincenzo; Prof Dr Cervelli Valerio.

E N D
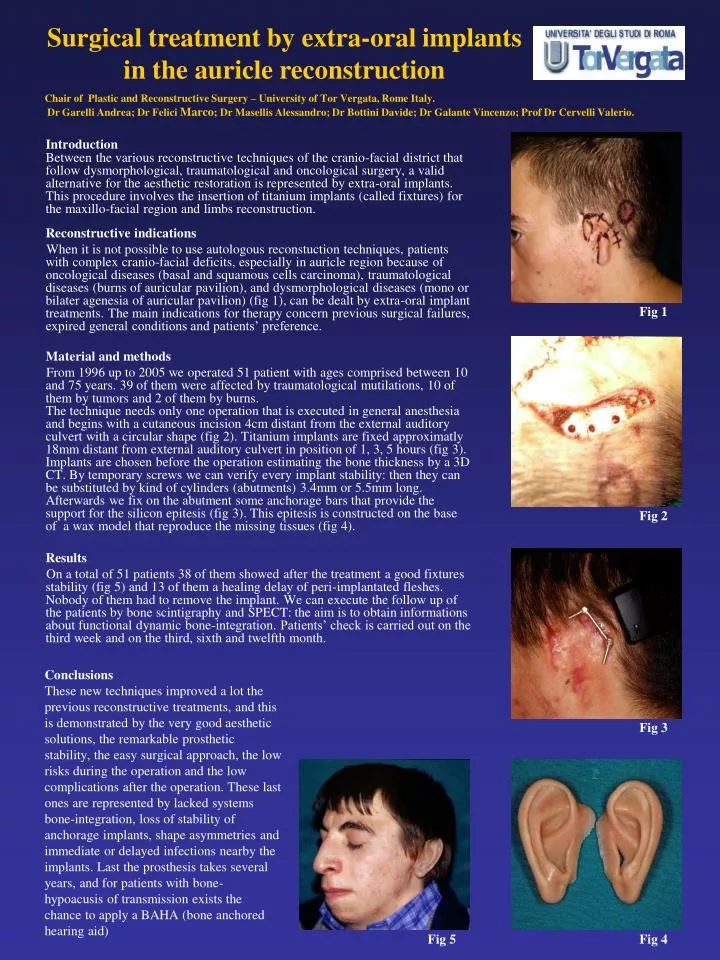
Surgical treatment by extra-oral implants in the auricle reconstruction Chair of Plastic and Reconstructive Surgery – University of Tor Vergata, Rome Italy. Dr Garelli Andrea; Dr Felici Marco; Dr Masellis Alessandro; Dr Bottini Davide; Dr Galante Vincenzo; Prof Dr Cervelli Valerio. Introduction Between the various reconstructive techniques of the cranio-facial district that follow dysmorphological, traumatological and oncological surgery, a valid alternative for the aesthetic restoration is represented by extra-oral implants. This procedure involves the insertion of titanium implants (called fixtures) for the maxillo-facial region and limbs reconstruction. Reconstructive indications When it is not possible to use autologous reconstuction techniques, patients with complex cranio-facial deficits, especially in auricle region because of oncological diseases (basal and squamous cells carcinoma),traumatological diseases (burns of auricular pavilion), and dysmorphological diseases (mono or bilater agenesia of auricular pavilion) (fig 1), can be dealt by extra-oral implant treatments. The main indications for therapy concern previous surgical failures, expired general conditions and patients’ preference. Material and methods From 1996 up to 2005 we operated 51 patient with ages comprised between 10 and 75 years. 39 of them were affected by traumatological mutilations, 10 of them by tumors and 2 of them by burns.The technique needs only one operation that is executed in general anesthesia and begins with a cutaneous incision 4cm distant from the external auditory culvert with a circular shape (fig 2). Titanium implants are fixed approximatly 18mm distant from external auditory culvert in position of 1, 3, 5 hours (fig 3). Implants are chosen before the operation estimating the bone thickness by a 3D CT. By temporary screws we can verify every implant stability: then they can be substituted by kind of cylinders (abutments) 3.4mm or 5.5mm long. Afterwards we fix on the abutment some anchorage bars that provide the support for the silicon epitesis (fig 3). This epitesis is constructed on the base of a wax model that reproduce the missing tissues (fig 4). Results On a total of 51 patients 38 of them showed after the treatment a good fixtures stability (fig 5) and 13 of them a healing delay of peri-implantated fleshes. Nobody of them had to remove the implant.Wecan execute the follow up of the patients by bone scintigraphy and SPECT: the aim is to obtain informations about functional dynamic bone-integration. Patients’ check is carried out on the third week and on the third, sixth and twelfth month. Fig 1 Fig 2 Conclusions These new techniques improved a lot the previous reconstructive treatments, and this is demonstrated by the very good aesthetic solutions, the remarkable prosthetic stability, the easy surgical approach, the low risks during the operation and the low complications after the operation. These last ones are represented by lacked systems bone-integration, loss of stability of anchorage implants, shape asymmetries and immediate or delayed infections nearby the implants. Last the prosthesis takes several years, and for patients with bone-hypoacusis of transmission exists the chance to apply a BAHA (bone anchored hearing aid) Fig 3 Fig 5 Fig 4