Download
1 / 24
680 likes | 2.12k Views
Orbital Cellulitis. Orbit anatomy. Frontal. Nasal. Ethmoid. Sphenoid. Lacrimal. Zygoma. Maxillary. Orbital Cellulitis. Orbital cellulitis is a dangerous infection with potentially serious complications. It is usually caused by a bacterial infection from

E N D
Orbit anatomy Frontal Nasal Ethmoid Sphenoid Lacrimal Zygoma Maxillary
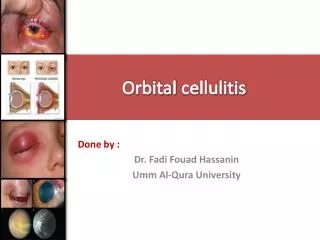
Orbital Cellulitis Orbital cellulitis is a dangerous infection with potentially serious complications. It is usually caused by a bacterial infection from the sinuses (mainly ethmoid, accounting for more than 90% of all cases) Other causes :a stye on the eyelid, recent trauma to the eyelid including bug bites, or a foreign object
Children In children, orbital cellulitis is usually from a sinus infection and due to the organism. Hemophilus influenza (decrease in incidence after vaccination program implantation). Other organisms are Staphylococcus aureus, Strep.pneumonia, and Beta. H streptococci
Pathophysiology Extension of infection from the periorbital structures, most commonly from the paranasal sinuses, but also from the face, globe, and lacrimal sac. Direct inoculation of the orbit from trauma or surgery (orbital decompression, DCR, eyelid surgery, strabismus surgery, retinal surgery, and intraocular surgery, have been reported as the precipitating cause of orbital cellulitis) Hematogenous spread from bacteremia.
Orbital septum The orbit is separated from the soft tissue of the eyelid by the orbital septum. This is a facial plane that is continuous with the periosteum of the facial bones. The orbital septum inserts into the tarsal plate of the upper and lower eyelids. The orbital septum usually proves to be an effective barrier that prevents the spread of infection from the eyelids posteriorly to the orbit. While preseptal cellulitis can occasionally spread to the orbital contents, it is generally a clinical entity that is distinct from orbital cellulitis
Orbital vs. Preseptal Cellulitis Orbital cellulitis is infection of the soft tissues of the orbit posterior to the orbital septum, differentiating it from preseptal cellulitis, which is infection of the soft tissue of the eyelids and periocular region anterior to the orbital septum DD: orbital pseudotumor (inflammatory condition, responds to steroids)
Chandler Classification Stage I Inflammatory edema-Preseptal Stage II Orbital cellulitis - Postseptal Stage III Subperiostal abscess Stage IV Orbital abscess Stage V Complication due to posterior extension
Symptoms Fever, generally 39 degrees C or greater. Eyelid appears shiny and is red or purple in color. Infant or child is acutely ill or toxic. Eye pain especially with movement. Decreased vision proptosis Painful swelling of the eyelids General malaise. Restricted or painful eye movements
Complications Subperiostal/Orbital abscess Cavernous sinus thrombosis Hearing loss Septicemia Meningitis Optic nerve damage and blindness
A male with orbital cellulitis with proptosis, ophthalmoplegia, eyelids edema and erythema .
Non-surgical treatment IV ABx Antifungal (if indicated) Nasal decongestants (open sinus ostia) Diuretics – DIAMOX (carbonic anhydrase inhibitor), manitol.
Surgical Treatment Surgical drainage if failed response to appropriate antibiotic within 48-72 h . Every case of subperiosteal or intraorbital abscess formation. Decrease V/A, RAPD. proptosis progresses despite appropriate antibiotic therapy The size of the abscess does not reduce on CT scan within 48-72 hours after appropriate antibiotics have been administered. If brain abscesses develop and do not respond to antibiotic therapy, craniotomy is indicated.
How? Superior orbit decompression Medial orbit decompression Inferior orbit decompression Lateral orbit decompression Intranasal approach
Superior Orbit Decompression Frontal cranioitomy – unroofing of superior wall of orbit Titanium sheild placed to support the frontal lobe of the brain High morbidity, consider only for severe cases
Medial Orbit Decompression External ethmoidectomy incision or coronal forehead approach External ethmoidectomy- complete ethmoid sinus resection, then orbital fat herniated into sinus defect Coronal incision- ethmoidectomy via a superior approach, more risk for lacrimal sac and trochlea injury
Inferior Orbit Decompression Orbital floor blow-out Fx ,but spares infraorbital nerve. Subciliary eyelid incision or Caldwell-Luc incision Combined approach? Intraorbital fat herniates maxillary sinus
Lateral Orbit Decompression Lateral canthotomy Removal of lat. orbital bone posterior to the rim Orbital fat protrudes the newly created space
An incision extending from the lateral canthus to the area just below the inferior punctum is created 4 mm to 5 mm below the lower border of the tarsal plate to avoid injury to the septum and the canaliculus
Intranasal approach Decompression of medial and medioinferior floors of orbit. Endoscopic sinus surgery technique. Anterior Ethmoidectomy Maxillary antrostomy