Download
1 / 48
480 likes | 581 Views
DEVELOPMENT OF WHO GUIDANCE FOR THE PREVENTION AND TREATMENT OF HIV/STI AMONG MSM AND TRANSGENDER PEOPLE. Antonio Gerbase, MD, MSc Medical Officer, The World Health Organization, Department of HIV/AIDS. Goal of this Presentation.

E N D
DEVELOPMENT OF WHO GUIDANCE FOR THE PREVENTION AND TREATMENT OF HIV/STI AMONG MSM AND TRANSGENDER PEOPLE Antonio Gerbase, MD, MSc Medical Officer, The World Health Organization, Department of HIV/AIDS
Goal of this Presentation To provide information on the context that led to the development of this guidance To describe the process for developing the WHO guidelines on health sector interventions for HIV and STI prevention and treatment among men who have sex with men (MSM) and transgender people To describe civil society's participation in this process.
Guidance Development One of WHO’s main tasks is to develop evidence-based technical guidance for clinical procedures and public health programs to inform health systems worldwide WHO is finalizing guidance for delivering an evidence-based, essential package of interventions for the prevention and treatment of HIV and other STI among MSM and transgender people. This guidance primarily targets the health sector (broadly defined) in low- and middle-income countries.
UNAIDS Action Framework:Universal Access for MSM and Transgender People (2008) • Three key principles: • Actions must be grounded in an understanding of, and commitment to, human rights • Action must be informed by evidence • Action is required by a broad range of partners, simultaneously addressing both short and long term needs and opportunities • Responsibilities • UNAIDS: Coordination and Evidence • UNDP: Gender and human rights • WHO: Response in the health sector
Role of WHO • WHO is the UNAIDS cosponsor responsible for promoting and supporting health sector initiatives. • WHO has established priorities under 5 strategies for action in critical areas where the health sector must invest if it is to make progress towards achieving universal access: 1. Enable people to know their HIV status 2. Maximize the health sector’s contribution to HIV prevention 3. Accelerate the scale-up of HIV/AIDS treatment and care 4. Strengthen and expand health systems 5. Invest in strategic information to guide a more effective response
HIV and Men who have Sex with Men and Transgender People • Global WHO consultation (2008) • Regional consultations, advocacy and tools • UN Framework for Action (2009) • UNAIDS business case (2010-11)
Set-up of the working group • As part of this process WHO instituted an informal, ad-hoc working group consisting of: • Public health experts, • Colleagues from other WHO departments and UN agencies • Researchers • Representatives of affected communities • …working in prevention and treatment of HIV and other STI among MSM and transgender people.
Technical Teams WHO, HIV Department: Ying-Lu Ro, Antonio Gerbase, Michelle Rodolph, Kevin O’Reilly UPCH: Carlos F. Caceres, Kelika Konda, Eddy Segura, Segundo León (and other colleagues) JHSPH: Caitlin Kennedy Cochrane Collaboration: Tara Horváth (PSG/UCSF), Charles Wysonge (UCT), and other colleagues. Global Forum on MSM & HIV: George Ayala and Sonya Arreola GRADE methodologist: Elie Akl Peer reviewers Working Group Members (advisory role)
The purpose of the guidance • Recommends a set of interventions for the prevention and treatment of HIV and other STI for MSM and transgender people
Principles Regional and country guidance A supportive environment and a human rights-based approach Continued political advocacy Partnerships and civil society involvement (affected community and people living with HIV) Biomedical, behavioural and structural interventions
Target Audience Public health officials and managers (HIV & STI) Implementers, such as NGOs and CBOs, working with affected communities. Health care providers Bi-lateral and multilateral donors The Global Fund for Fighting AIDS, TB and Malaria
Timeline and key steps to develop the guidance 7. Identify Guideline Consensus Group (chair, consensus group, peer reviewers) 1. Scope the work 2009 Sep-Dec '09 2. Formulate questions and choices of relevant outcomes 3. WHO Guideline Committee Approval Jan '10 4. Retrieve evidence, evaluate and synthesize Feb - May '10 5. First informal working group meeting, Washington Apr '10 6. Prepare GRADE profiles & risk benefit tables & recommendations May – Jun '10 May'10 8.Second informal working group meeting, Geneva Jun '10 9. Civil society consultation Jul '10 10. External peer review Aug '10 11. Global guideline consensus meeting China Sep '10 Oct '10 – Feb 11 12. Drafting – Comments – Peer review 12. Approval – Launching - Dissemination Mar – Jun '11
Guidance development process • Topic identification • Existing guidance? Existing guidelines outdated? • Literature review • Formulate search (PICO) questions • Evidence retrieval • Evidence GRADEd • Community consultation • Expert discussion: • Risks and benefits • Community values and preferences • Consensus meeting to agree on recommendations • All process under oversight of WHO Guideline Review Commitee
Methods of Guidance Development WHO follows the GRADE approach for the development and review of recommendations. GRADE process requires consultation with different partners, including end-users of interventions. Global Forum on MSM & HIV conducted a values and preferences study. A civil society consultation process, on-line and face-to-face, sought feedback from community stakeholders.
GRADE Working Group Grades of Recommendation Assessment, Development and Evaluation CMAJ 2003, BMJ 2004, BMC 2004, BMC 2005, AJRCCM 2006, Chest 2006, BMJ 2008, Lancet ID 2007, PLOS Medicine 2007
Recommendation A recommendation should provide a clear and specific answer to a specific question raised by the target users Specific questions are formulated as PICO questions: P: population I: intervention C: comparator O: outcomes
Structure of a recommendation Statement that addresses the elements of PICO question Grade the strength of recommendation Rate the quality of supporting evidence 19
Level of evidence • High - Further research is very unlikely to change our confidence in the estimate of effect. • Moderate - Further research is likely to have an important impact on our confidence in the effect. • Low - Further research is very likely to have an estimate of effect and is likely to change the estimate. • Very low - Any estimate of effect is very uncertain.
Strenghth of recommendation • A strong recommendation is one for which the desirable effects of adherence to a recommendation outweigh the undesirable effects. • A conditional recommendation is one for which the desirable effects of adherence to a recommendation probably outweigh the undesirable effects. However, data to support the recommendation are scant.
Types of recommendations A recommendation can have one of 2 directions: In favor Against As a result there are 4 combinations of strength and direction for a recommendation: Strong in favor of the intervention Conditional in favor of the intervention Conditional against the intervention Strong against the intervention
Values and preferences The greater the variability in values and preferences, or uncertainty in values and preferences, the more likely a conditional recommendation is warranted. In some cases, certain values and preferences might lead to strong recommendations 23
Values and Preferences: Interview Guide • Management of the sexual health needs of MSM and transgender people in your country? • Experience with prevention programs? • Condoms and lubricants • Individual/group/community-level interventions • Testing and counseling for HIV and STI • Risk reduction counseling • Experience with STI screening? • Experience with HIV &STI services? • Decision making about having sex based on the HIV status of their partners by MSM transgender people? • View of circumcision in your country? • Treatment of MSM and transgender people in your country?
Risk benefit tables Summarize the factors that affect the strength of recommendation: Quality of evidence Balance of benefits and harms Values and preferences Resource use 25
Framework for the prevention and treatment of HIV and other STIs for men who have sex with men and transgender people 1.Biomedical interventions 3. Enabling environment 5. Other interventions Condoms STI control Testing & Counselling ART Anti-discrimination Protective laws Hepatitis vaccination Alcohol, psychostimulants Medical ethics Harm reduction 4. Communication Individual level behavioral interventions Community level behavioral interventions Safe injections Internet / phone Sex venues Social marketing 2. Behavioral interventions
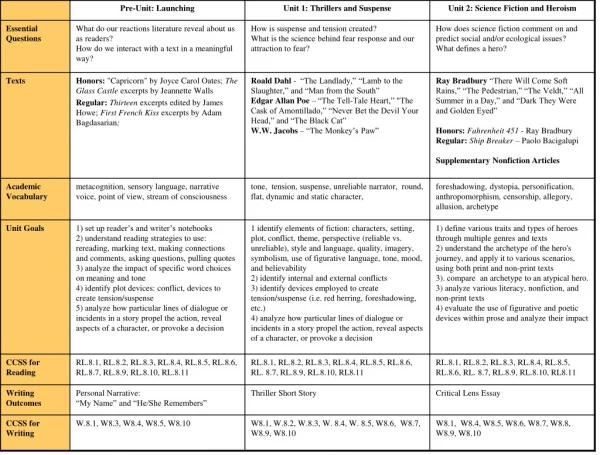
Areas • Good practices (2) • Individual sexual behaviour (2) • Testing and counselling (2) • Behavioural interventions and novel strategies of communication (5) • Mental health, harm reduction and male circumcision (4) • HIV treatment and care (2) • Sexually Transmitted Infections (4)
Good Practice Recommendations • Human Rights and inclusive environments • Non-discrimination in health care settings and medical ethics
Evidence and Technical Recommendations • Individual sexual behaviour • HIV testing and counselling • Behavioural interventions and information, education, communication • Substance use, prevention of blood-borne infection, male circumcision • HIV care and treatment • STI prevention and care
I. Good practices • We recommend that legislators and other government authorities establish anti-discrimination and other protective laws, derived from international human rights standards, in order to eliminate discrimination and violence faced by men who have sex with men and transgender people, in order inter alia to reduce their vulnerability to infection with HIV and the impacts of HIV and AIDS. • We recommend making health services inclusive of men who have sex with men and transgender people, based on the principles of medical ethics and the right to health.
II. Individual sexual behaviour • Using condoms consistently during anal intercourse is strongly recommended over not using condoms among MSM and transgender people. • Strong recommendation, moderate quality evidence • Using condoms consistently is strongly recommended over serosorting for HIV-negative MSM and transgender people. • Strong recommendation, very low quality evidence • Serosorting is suggested over not using condoms among HIV-negative MSM and transgender people under specific circumstances as a harm reduction strategy. • Conditional recommendation, very low quality evidenc
III. Testing and counselling • Offering HIV testing and counselling is strongly recommended over not offering such intervention for MSM and transgender people. • Strong recommendation, low quality evidence. • Offering community-level programs for HIV testing and counselling linked to care and treatment is suggested over not offering such programs to MSM and transgender people. • Strong recommendation, very low quality evidence.
IV. Behavioural interventions and novel strategies of communication(a) • Implementing individual-level behavioural interventions for the prevention of HIV and STIs is suggested over not implementing such interventions among MSM and transgender people. • Conditional recommendation, moderate quality evidence. • Implementing community-level behavioural interventions for the prevention of HIV and STIs is suggested over not implementing such interventions among MSM and transgender people. • Conditional recommendation, low quality evidence.
IV. Behavioural interventions and novel strategies of communication(b) • Offering targeted internet-based targeted information to decrease risky sexual behaviours and increase uptake of HIV testing is suggested over not offering such information among MSM and transgender people. • Conditional recommendation, very low quality evidence. • Using social marketing strategies to increase uptake of HIV/STI testing and HIV services is suggested over not using such strategies among MSM and transgender people. • Conditional recommendation, very low quality evidence. • Implementing sex venue-based outreach strategies to decrease risky sexual behaviour and increase uptake of HIV testing is suggested over not implementing such strategies among MSM and transgender people. • Conditional recommendation, very low quality evidence.
V.Mental health, harm reduction and male circumcision(a) • MSM and transgender people with harmful alcohol or other substance use should have access to evidence based brief psychosocial interventions, involving assessment, specific feedback and advice. • In line with existing WHO guidance • MSM and transgender people who inject drugs should have access to needle and syringe programs and opioid substitution therapy. • In line with existing WHO guidance
V.Mental health, harm reduction and male circumcision (b) • Transgender people who inject substances for gender enhancement should use clean injecting equipment and practice safe injection to reduce the risk of infection with blood borne pathogens such as HIV, hepatitis B and hepatitis C. • In line with existing WHO guidance • Not offering adult male circumcision for the prevention of HIV and STI is suggested over offering it to MSM and transgender people. • Conditional recommendation, very low quality evidence.
Antiretroviral therapy • Antiretroviral treatment recommendations for adults and adolescents apply to MSM and transgender people • WHO 2010 revision
VI. HIV treatment and care • MSM and transgender people living with HIV should have access to ART the same as other populations. ART should be initiated at CD4 counts of ≤350 cells/mm3 (and for those with WHO clinical stage 3 or 4 if CD4 testing is not available) Access should also include management of opportunistic infections, co-morbidities and management of treatment failure • In line with existing WHO guidance • MSM and transgender people living with HIV should have access to essential interventions to prevent illness and HIV transmission, including but not limited to care and support, testing and counselling and antiretroviral therapy. • In line with existing WHO guidance
Follow flow charts as per WHO STI management guidelines Management of symptomatic STIs
VII. Sexually Transmitted Infections (a) • MSM and transgender people with symptomatic STI's should seek and be offered syndromic management and treatment • In line with existing WHO guidance • Offering periodic testing for asymptomatic urethral and rectal Chlamydia trachomatis infections using NAAT is suggested over not offering such testing for MSM and transgender people. • Conditional recommendation, low quality evidence • Not offering periodic testing for asymptomatic urethral and rectal Neisseria gonorrhoea infections using culture is suggested over offering such testing for MSM and transgender people. • Conditional recommendation, low quality evidence
VII. Sexually Transmitted Infections (b) • Offering periodic serologic testing for asymptomatic syphilis infection is strongly recommended over not offering such screening for MSM and transgender people. • Strong recommendation, moderate quality evidence. • MSM and transgender people should be included in catch-up HBV immunization strategies in settings in which infant immunization has not reached full coverage. • In line with existing WHO guidance
Summary of recommendations - I • To establish anti-discrimination and other protective laws • To make health services inclusive of men who have sex with men and transgender people • To use condoms during anal intercourse. MOD • To use of condoms is recommended over serosorting. VERY LOW • Serosorting is suggested over not using condoms under specific circumstances. VERY LOW • To offer HIV testing and counselling. LOW • To offer community-level programs for HIV testing and counselling linked to care. VERY LOW • To implement individual-level behavioural interventions. MOD • To implement community-level behavioural interventions. LOW
Summary of recommendations - II • To offer targeted internet-based targeted information.VERY LOW • To using social marketing strategies. VERY LOW • To implement sex venue-based outreach strategies. VERY LOW • MSM and transgender people with harmful alcohol or other substance use should have access to evidence based brief psychosocial interventions • MSM and transgender people who inject drugs should have access to needle and syringe programs and opioid substitution therapy. • Transgender people who inject substances for gender enhancement should use clean injecting equipment and practice safe injection • Do not offering adult male circumcision for the prevention of HIV and STI to MSM and transgender people.VERY LOW
Summary of recommendations - III • To have access to ART the same as other populations • To have access to essential interventions to prevent illness and HIV transmission • To seek and be offered syndromic management and treatment of STIs • To offer periodic testing for asymptomatic urethral and rectal Chlamydia trachomatis infections using NAAT. LOW • Do not offer periodic testing for asymptomatic urethral and rectal Neisseria gonorrhoea infections using culture. LOW • To offer periodic serologic testing for asymptomatic syphilis infection. MOD • To include in catch-up HBV immunization strategies
Thank you Note: The guidelines' recommendations are in the process of final aproval. We are sharing the content with the aim to inform all participants. We thank you for not disseminating the recommendations before the formal launching.