Download

1 / 18
680 likes | 2.53k Views
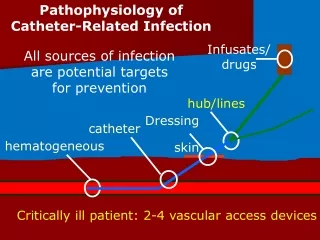
VASCULAR ACCESS DEVICES. VASCULAR ACCESS DEVICES. Introduced in early 1980s Allow medications to be delivered directly into larger veins Less likely to clot Can be left in for longer periods of time. TYPES OF VASCULAR ACCESS. Central Venous Catheters Tunneled CVC’s: Hickman Broviac

E N D
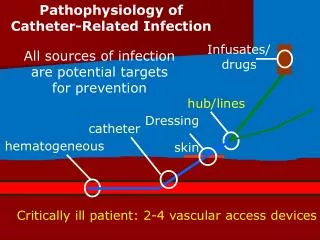
VASCULAR ACCESS DEVICES Introduced in early 1980s Allow medications to be delivered directly into larger veins Less likely to clot Can be left in for longer periods of time
TYPES OF VASCULAR ACCESS • Central Venous Catheters • Tunneled CVC’s: • Hickman • Broviac • Groshong • Percutaneous CVC’s: • Ports • PICC Lines • Fistulas
TUNNELED CATHETERS Surgically inserted Tunnel made through subcutaneous tissue (usually b/t clavicle and nipple) Tip inserted through cephalic, internal or external jugular and threaded into superior vena cava Held in place with Dacron cuff under skin Placement verified through x-ray Can be single, double or triple lumen
Tunneled catheters Placement of Tunneled Catheters Tunneled Catheters
PERCUTANEOUS CATHETERS -PORTS First used in oncology patients in 1981; now 100,000 ports implanted yearly Surgically implanted beneath skin, usually in chest region Right side of chest preferable d/t anatomy (superior vena cava) – “kangaroo” pocket created for portal body Accessed by IP, Huber, or other type of needle with deflective, non-coring tip
PORTS Placement of ports Port Images
Reasons for Ports • Long term IV therapy • Frequent blood transfusions or blood draws • Bone marrow transplant • Protection of smaller vessels
Ports • Advantages • Decreased chance of infection – port sealed under skin • Less interference with ADLs – no external components • Less body image concerns (teens) • Long usable life – up to 10 years (compared to <1 yr for PICC line) • Disadvantages • Needle access • Most expensive device to place • Requires minor surgical procedure for placement • Can be difficult for patients to maintain
PERCUTANEOUS CATHETERS -PICC LINES PICC – Peripherally Inserted Central Catheter Inserted in interventional radiology or patient room by: Physician Physician Assistant Nurse Practitioner Certified PICC nurse specialist Placed in peripheral vein (basilic, cephalic or brachial) and advanced into superior vena cava or cavo-atrial junction
PICC LINES Healthcare providers often use ultrasound for placement followed by x-ray (fluoroscopy)to assure proper placement
Reasons for PICC Lines • Reduced number of needle punctures • Prolonged IV antibiotic treatment • TPN nutrition • Chemotherapy • Repeated administration of blood or blood products • Venous blood samples • Measurement of central venous pressure
FISTULAS Used for dialysis in patients with renal impairment Surgeon joins an artery and vein, bypassing capillaries, allowing blood to flow rapidly through the fistula Created in the non-dominant arm If vein quality is poor, grafts can be used Takes approximately 4-6 weeks to mature
FISTULAS Formation of fistulas Aneurysm of fistula
FISTULAS Radiocephalic • Most common fistula for hemodialysis • Created in forearm near wrist • Radial artery anastomosed to cephalic vein • Often created if poor lower arm vessels or after failure of radiocephalic fistula • Created in arm near elbow • Brachial artery anastomosed to cephalic vein Brachiocephalic
FISTULAS • Benefits: • Lower infection rates • Higher blood flow rates = more effective dialysis • Lower incidence of thrombosis • Complications: • “Steal syndrome” = cold limb, cramping, tissue damage • Aneurysm d/t repeated needle insertion • Thrombosis • Failure to mature
DIALYSIS Two needles inserted into fistula, one to draw blood, one to return it
References • Bartholomay, M., Dreher, D., Evans, T., Finn, S., Guthrie, D., Lyons, H., Mulligan, J., & Tyksienski, C. (n.d.) Nursing management of venous access devices: Non-tunneled catheters. Retrieved from http://www.mghpcs.org/EED_Portal/Documents/Central_Lines/CL_Module7.pdf • Nursing Link (2012). The use and maintenance of implanted port vascular access devices. Retrieved from http://nursinglink.monster.com/training/articles/302-the-use-and-maintenance-of-implanted-port-vascular-access-devices • Queensland Vascular (n.d.) Vascular and endovascular surgery. Retrieved from http://www.qldvascular.com.au/renal-clinic.html • Roe, E. J., III, & Turner-Lawrence, D. (2012). Central venous access via subclavian approach to the subclavian vein. Retrieved from http://emedicine.medscape.com/article/80336-overview