Download
1 / 28
300 likes | 701 Views
MEDIAL RECTUS PULLEY SUTURE : PRELIMINARY EXPERIENCE . LIONEL KOWAL ELINA LANDA RVEEH MELBOURNE. ‘FADEN SUTURE’ . Many synonyms Long history: Germany 50 yrs ago Frequently used in European and Latin strabismus Lower acceptance in Anglo- American strabismus. MECHANISM OF FADEN .

E N D
MEDIAL RECTUS PULLEY SUTURE : PRELIMINARY EXPERIENCE LIONEL KOWAL ELINA LANDA RVEEH MELBOURNE
‘FADEN SUTURE’ • Many synonyms • Long history: Germany 50 yrs ago • Frequently used in European and Latin strabismus • Lower acceptance in Anglo- American strabismus
MECHANISM OF FADEN • Previous: change tangent of action of muscle • Demer: major mechanism - create restriction of movement through the pulley • New intra-operative end point: restriction SEMINAL PAPER R A. Clark, J L. Demer Posterior fixation sutures: a revised mechanical explanation for the fadenoperation …. Am J Ophth 1999
COMMON USE : TO COMPENSATE FOR INCOMITANCE • MR: Desired Effect: to have no effect on primary position, and to only effect ADduction. Typically used to augment effect of MR recess esp for convergence Xs. • SR: to augment effect of SR recess in DVD • IR: ..after contralateral blowout
Normal Adduction MR insertion A PULLEY If we want to impair Adduction without affecting primary position… Medial orbital wall B A, B : ant & post extent of pulley sleeve
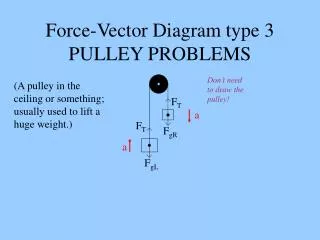
Scleral suture after Demer Primary gaze 18 degrees ADd P = scleral suture MR insertion A A PULLEY P 18º P B Medial orbital wall Adduction restricted by P B MR MR A, B : ant & post extent of pulley sleeve
SCLERAL FADEN • Many different techniques - all seem to work similarly RARE COMPLICATIONS • Perforation • Scarring ant to suture
THE NEW FADEN: PULLEY SUTURE • Technically difficult - the surgical anatomy of the pulley is NOT well definedeven though radiological / histological anatomy is From Clark & Demer
THE NEW FADEN: PULLEY SUTURE • Create restriction of movement through pulley by suturing muscle to the pulley • Theoretically safer - no scleral suture • Technically difficult • [so far] not titratable *: Will this one have a ‘small’ or ‘large’ effect? * similar with scleral Faden • No long term results
Normal Adduction MR insertion A PULLEY If we want to impair Adduction without affecting primary position… Medial orbital wall B A, B : ant & post extent of pulley sleeve
Diagrams of pulley suture P Primary gaze 18 degrees ADd P = pulley suture MR insertion A A PULLEY P P B Medial orbital wall LR B MR MR A, B : ant & post extent of pulley sleeve
9 pts : standard BMR + scleral faden: 2 – only scleral faden 7 – BMRc + scleral faden Postoperatively: 6/9 – imroved stereoacuity 8/9 – no longer needed bifocals D/N disparity av of 12∆ 13 pts : BMR pulley sutures: 3 – only pulley suture 10 – BMR +pulley suture Postoperatively: 8/13 – improved stereoacuity 12/13 – no longer needed bifocals D/N disparity av of 14∆ Medial rectus pulley posterior fixation is as effective as scleral posterior fixation for acquired ET with high AC/A R A. Clark, J L. Demer Am J Ophthalmol 2004
Medial rectus pulley posterior fixation: a novel technique to augment recessionR A. Clark, R Ariyasu, J L. Demer JAAPOS 2004 • 16 pts : standard Rs and/or Rc operations with MR pulley fixation: - 9 pts – recurrent ET with conv Xs 5 – BMR re-Rc + BMR pulley suture 4 – MR re-Rc + pulley suture +ipsi LR Rs Postoperatively, D/N disparity decreased av of 11∆. All pts : Dist ET ≤ 10 ∆. No pt overcorrected.
2007 / 2008 • 2007: 7 patients • 2008: now 15 • 1 abandoned PS [ scleral faden] • Longer follow up on some ‘07 patients
Types of patients for PS • 1. Variable ET n=3 • 2. Convergence Xs n=7 • 3. Adding PS to previous BMR n=2 • 4. Adding PS for anticipated poor gls compliance n=1 • 5. PS for face turn of LMLN n=1 • 6. Conv Xs in sensory ET n=1
#1 44681 • CET onset 6mo. Presents @ 22mo. • Delivered 33w • L amblyopia ; atropine [i/mitt R ET] and patching • Cyclo +1 DS OU • ET 0-40, av 5. ET’ 40-73 av. 57 [12 visits] • Frequent L face turn • Rx: pulley sutures
#1 POST OP • ET 0-15, av 1.5 • ET’ 0-45, av 27 [n=9]…was 57! • BMR 4.5 • 3 mo: EX=0, ET’ 15 • 8 mo: EX / EX’ = 0. LMLN with alternating face turns • Pulley sutures inadequate as only Rx for huge conv Xs in CET, but can add BMR as a 2ary procedure.
Variable ET • 2 further pts with variable ET • BMR + PS effective • Dose of BMR: • 1. Recent D angle • 2. Average D angle
Types of patients for PS • 2. Convergence Xs n=7 • 1. Variable ET n=3 • 3. Adding PS to previous BMR n=2 • 4. Adding PS for anticipated poor gls compliance n=1 • 5. PS for face turn of LMLN n=1 • 6. Conv Xs in sensory ET n=1
Convergence Xs • BMR + PS is a very convincing operation in this small series • Selection bias: • V. lge ET’ [60,60,85] • V. lge N>D [15,30,20,40+,20] • Small D [0, 6-14]
Types of patients for PS • 1. Convergence Xs n=7 • 2. Variable ET n=3 • 3. Adding PS to previous BMR n=2 • 4. Adding PS for anticipated poor gls compliance n=1 • 5. PS for face turn of LMLN n=1 • 6. Conv Xs in sensory ET n=1
Adding PS to previous BMR for persisting conv Xs • N=2 • 1 worked very well • 1 didn’t work @ all
Types of patients for PS • 1. Convergence Xs n=7 • 2. Variable ET n=3 • 3. Adding PS to previous BMR n=2 • 4. PS for face turn of LMLN n=1: poor • 5. Adding PS to BMR for ET with anticipated poor gls compliance n=1: Great • 6. Conv Xs in sensory ET n=1: poor
FAILED PULLEY SUTURES • #1 after previous RMR Rs. Used scleral Faden: good result
Pulley suture • 15 pts with variable ET or marked conv XS • More difficult than scleral faden • No long term outcomes Promising for: • Variable ET • Conv Xs • Where gls wear unlikely
Pulley suture : the future • How much intraop restriction is enough?…too much? Need scheme for intraoperative control of acquired restriction & correlation with postop result • No long term results - scleral faden has 50 y history. Does PS fall apart after x years? • Long term status of pulley vs scleral suture : clinical data and histology req’d