Download
1 / 62
620 likes | 785 Views
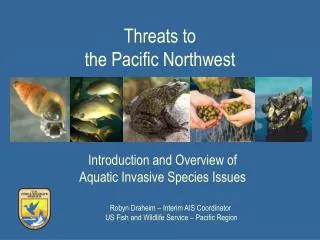
PSYCHOPHARMACOLOGICAL APPROACHES TO NEUROBEHAVIORAL IMPAIRMENT FOLLOWNG ABI THIRD ANNUAL PACIFIC NORTHWEST BRAIN INJURY CONFERENCE. NATHAN D. ZASLER, MD CEO & MEDICAL DIRECTOR, CONCUSSION CARE CENTRE OF VIRGINIA AND TREE OF LIFE SERVICES CLINICAL PROFESSOR, DEPT. OF PM&R, VCU

E N D
PSYCHOPHARMACOLOGICAL APPROACHES TO NEUROBEHAVIORAL IMPAIRMENT FOLLOWNG ABITHIRD ANNUAL PACIFIC NORTHWEST BRAIN INJURY CONFERENCE NATHAN D. ZASLER, MD CEO & MEDICAL DIRECTOR, CONCUSSION CARE CENTRE OF VIRGINIA AND TREE OF LIFE SERVICES CLINICAL PROFESSOR, DEPT. OF PM&R, VCU CLINICAL ASSOC. PROFESSOR, DEPT. OF PM&R, UVA
PSYCHOPHARMACOLOGIC PRACTICES IN TBI • NO FDA APPROVED TREATMENTS FOR COGNITIVE OR BEHAVIORAL IMPAIRMENTS DUE TO TBI • PHARMACOTHERAPIES ARE GENERALLY MODELED AFTER THOSE FOR PATIENTS WITH PHENOMENOLOGICALLY SIMILAR BUT ETIOLOGICALLY DISTINCT DISORDERS
GENERAL GUIDELINES • MINIMIZE POLYPHARMACY • KNOW YOUR DRUGS • CONSIDER ALTERNATE CHOICES • START LOW, GO SLOW • TITRATE BASED ON RESPONSE • BRING MEDICATIONS OR LIST • REVIEW REGULARLY • EDUCATE
RULE FOR PRESCRIBERS • KNOW DRUG PROS AND CONS • KEEP UP WITH LITERATURE – IN GENERAL AND IN ABI • REMEMBER COST, COMPLIANCE AND QOL ISSUES • ASK, LISTEN, EDUCATE AND BE RESPONSIVE • MONITOR, MEDIATE AND MODULATE • ASSESS AND TREAT HOLISTICALLY • DO NOT TREAT IMPAIRMENTS IN ISOLATION OF FUNCTIONAL DISABILITIES
QUESTIONS THAT SHOULD BE ASKED • WHAT DRUGS HAVE BEEN TRIED • WHAT WAS DURATION OF TREATMENT • WHAT DRUG DOSAGE WAS USED • WHY WAS DRUG PRESCRIBED IN FIRST PLACE • WHAT WERE DRUG TREATMENT GOALS
DRUG SIDE-EFFECTS • ALL DRUGS HAVE SIDE-EFFECTS • SOME ARE BENIGN, SOME CAN BE FATAL • WITHDRAWAL VS. DISCONTINUATION SYNDROMES • IF YOU DON’T ASK YOU WON’T KNOW (E.G. SEXUAL PROBLEMS)
DRUG SIDE-EFFECTS • DRUG INSERTS – DO’S & DON’TS • DOCS DON’T KNOW EVERYTHING • NEUROPSYCHIATRIC PATIENTS SHOW INCREASED FREQUENCY AND SEVERITY OF SIDE-EFFECTS • CAN MANIFEST AS WORSENING OF NEUROLOGICAL SYMTPOMS
BEHAVIORAL ASSESSMENT MAY BE COMPROMISED BY: • IMPAIRED ATTENTION AND CONCENTRATION • IMPAIRED PLANNING AND PROBLEM SOLVING • IMPAIRED MEMORY AND LEARNING • IMPAIRED LANGUAGE FUNCTION
BEHAVIORAL ASSESSMENT AND COMMUNICATION DEFICITS • PROPOSITIONAL AND PROSODIC FUNCTION CAN BE IMPAIRED • DIFFICULT TO MATCH AFFECT AND CONTENT • DENIAL SYNDROMES • LACK OF EXPERIENCE WITH PSYCHIATRIC LANGUAGE
FILTER EFFECTS OF CNS INJURY • WHAT DOES DEPRESSION LOOK LIKE IN SOMEONE WHO IS NON-VERBAL? • WHAT DOES MANIA LOOK LIKE IN SOMEONE WHO IS QUADRIPARETIC OR EVEN WORSE LOCKED-IN? • HOW DO HALLUCINATIONS AND DELUSIONS PRESENT IN SOMEONE WHO CANNOT ADEQUATELY DESCRIBE THEM DUE TO DYSPHASIA?
VULNERABILITY TO SIDE-EFFECTS • NEUROPSYCHIATRIC PATIENTS SEEM TO SHOW AN INCREASED FREQUENCY AND SEVERITY OF SIDE-EFFECTS TO MOST PSYCHOTROPICS • SIDE=EFFECTS CAN MANIFEST AS WORSENING OF NEUROLOGICAL SYMPTOMS: DYSARTHRIA, TREMOR, BRADYKINESIA, DECREASED COGNITION AND/OR BEHAVIOR
NEUROBEHAVIORAL TREATMENT APPROACHES • IDENTIFY THE MOST SALIENT BEHAVIORAL SYMPTOM CLUSTER • DECIDE IF THE PATTERN IS ANALOGOUS TO A MORE TYPICALLY DRUG RESPONSIVE SYNDROME • USE AS A RATIONAL GUIDE TO THERAPY
EXAMPLES OF METAPHORS: • “Depressive” Irritable, pessimistic, sad, weepy, socially withdrawn, vegetative features • “Psychotic” Angry when approached, overly suspicious, fragmented speech/thinking • “Manic” Euphoric, irritable, accelerated, hypersexual, reduced sleep
STUFF DOCS FORGET • ALCOHOL • CAFFEINE • NICOTINE • OTC MEDICATIONS • NATUROPATHIC AGENTS • HOMEOPATHIC AGENTS • ILLICIT DRUGS
DRUG TREATMENT IN ABI: CLASS EVIDENCE • PSYCHOSTIMULANTS • DOPAMINE AGONISTS • CHOLINOMIMETICS • SEROTONERGIC AGONISTS
PSYCHOSTIMULANTS • 10 CONTROLLED STUDIES WITH METHYLPHENIDATE - 6 WITH COGNITION • MAJORITY OF STUDIES DEALING WITH COGNITION SHOWED POSITIVE EFFECT FROM MP • IMPROVEMENTS IN SUSTAINED ATTENTION, PROCESSING SPEED AND DISTRACTIBILITY
PSYCHOSTIMULANTS • NO CONVINCING EVIDENCE THAT MP HAS A PRIMARY BENEFICIAL EFFECT ON MEMORY • EFFECT ON MOOD AND BEHAVIOR GENERALLY IN POSITIVE DIRECTION • MP DOES NOT APPEAR TO AFFECT MOTOR SPEED • MP MAY ENHANCE RATE OF NEURAL RECOVERY BUT NOT ULTIMATE PLATEAU
PSYCHOSTIMULANTS • ONLY 2 CONTROLLED STUDIES IN BI WITH DEXTROAMPHETAMINE • IMPROVES COGNITIVE PROCESSING SPEED • NO GOOD DATA ON MEMORY OR MOOD/BEHAVIOR EFFECTS
DOPAMINE AGONISTS • AMANTADINE IS BEST STUDIED OF ALL COMMONLY USED AGENTS • INCONSISTENT EFFECTS BUT GENERALLY FACILITATE ATTENTION, CONCENTRATION AND MODULATE BEHAVIOR • MAY MODULATE FRONTAL LOBE IMPAIRMENTS • DRUG CLASS OF CHOICE IN AM • CLASS AS A WHOLE USED MOST FREQUENTLY TO FACILITATE NEURORECOVERY IN MCS AND MODULATE BRADYKINETIC SYMPTOMS
CHOLINOMIMETICS • ALTHOUGH THERE ARE SEVERAL AGENTS IN CLASS NONE HAVE BEEN WELL STUDIED IN ND-ABI • DONEPEZIL IS BEST STUDIED AGENT IN TBI • NEWER AGENTS APPEAR MORE PROMISING THAN OLDER ONES (E.G. TACRINE) DUE TO SPECIFICITY AND SIDE-EFFECT PROFILE • MAY HAVE BOTH COGNITIVE AND BEHAVIORAL BENEFITS
SEROTONERGIC AGONISTS • LIMITED STUDIES EXIST IN TBI • GENERALLY WELL TOLERATED • LIKELY EFFECTIVE FOR A VARIETY OF BEHAVIORAL SPECTRUM DISORDERS • CARE NEEDS TO BE TAKEN WHEN COMBINING AGENTS AND/OR WITHDRAWING DRUG
COMMON PSYCHOSTIMULANT DRUGS AND DOSING • METHYLPHENIDATE: 2.5 - 5 BID, MAX 20 TID • AMPHETAMINE & DEXTROAMPHETAMINE: 5 QDAY, MAX 60/DAY (SPLIT) • DEXTROAMPHETAMINE: 5 QDAY, MAX 60/DAY (SPLIT) • PEMOLINE: 18.75 - 37.5 QDAY, MAX 112.5/DAY
COMMON DOPAMINERGIC DRUGS AND DOSING • L-DOPA/CARBIDOPA: 10 - 25 TID • AMANTADINE HCL: 50 BID, MAX 200 BID • BROMOCRIPTINE: 2.5 BID, MAX 40 TID • PERGOLIDE: .05/DAY, 5 MG/DAY (TID) • ROPINIROLE: .25 TID, MAX 24/DAY • PRAMIPEXOLE: .125 TID, MAX 1.5 TID • SELEGELINE:5 QDAY, MAX 5 BID
COMMON CHOLINOMIMETIC DRUGS AND DOSES • DONEZEPIL: 5/DAY, MAX 10/DAY • RIVASTAGMINE: 1.5 BID, MAX 6 BID • GALANTAMINE: 4 BID, MAX 12 BID • CDP-CHOLINE: 250 BID, MAX 1000 BID
COMMON PROSEROTONERGIC DRUGS AND DOSES • AMITRYPTILINE: 10 QHS, MAX 300/DAY • NORTRIPTYLINE: 10 QHS, 150/DAY IN DIVIDEDED DOSES • PROTRIPTYLINE: 5 QDAY, MAX20 TID • DOXEPIN: 10 QHS, MAX 300/DAY • IMIPRAMINE: 10 QHS, MAX 300/DAY
COMMON PROSEROTONERGIC (SSRI) DRUGS AND DOSES • FLUOXETINE: 10 QDAY, MAX 90/DAY • PAROXETINE: 10 QDAY, MAX 50/DAY • SERTRALINE: 50/DAY, MAX 200/DAY • FLUVOXAMINE:50 QHS, MAX 300/DAY • CITALOPRAM: 10/DAY, MAX 60/DAY • ESCITOLOPRAM: 10/DAY, MAX 20
OTHER ANTIDEPRESSANTS • VENLAFAXINE: 37.5 QDAY, MAX 375/DAY • BUPROPRION: 75/DAY, MAX 450/DAY • DULOXETINE: 20/DAY, MAX 60/DAY • TRAZODONE: 50/DAY, MAX 600/DAY • NEFAZODONE: 50/DAY, MAX 300 BID • MIRTAZAPINE: 15/DAY, MAX 45/DAY
ANTIPSYCHOTIC DRUGS AND DOSING • HALOPERIDOL: .5 BID, MAX 100/DAY • THIORIDAZINE: 50 TID, MAX 800/DAY • RISPERDONE: 1 BID, MAX 4 BID • QUETIAPINE: 25 BID, MAX 800/DAY • OLANZAPINE: 2.5/DAY, MAX 20/DAY • ZIPRASIDONE: 20 BID, MAX 80 BID
PSYCHOTROPIC ANTICONVULSANTS AND DOSES • VALPROIC ACID: 15 MG/KG, MAX 60/MG/KG • TOPIRAMATE: 25 QHS, MAX 400 BID • LAMOTRIGINE:50 QDAY, MAX 250 BID • OXCARBAZEPINE: 300 QDAY, MAX 1200 BID • GABAPENTIN: 10 MG/KG, 1200 TID • ZONISAMIDE: 50/DAY, MAX 300 BID • LEVETIRACETAM: 500 BID, 1500 BID
ANTIANXIETY DRUGS AND DOSES • BUSPIRONE: 7.5 BID, MAX 30 BID • ALPRAZOLAM: .25 TID, MAX 4/DAY • CLONAZEPAM: .5 QDAY, MAX 20/DAY • SSRIs - SEE PRIOR SECTION
MISCELLANEOUS DRUGS AND DOSES • PROVIGIL: 100 QDAY, 200 BID • ZOLPIDEM: 5 QHS, MAX 10 QHS • ZALEPLON: 5 QHS, MAX 20 QHS • LITHIUM: 300 QDAY, MAX DOSE = DOSE NEEDED TO ACHIEVE LEVEL OF .6 – 1.2 • NALTREXONE: 50 QDAY, MAX 100 QDAY
DIFFERENTIAL DIAGNOSIS OF BEHAVIORAL DYSFUNCTION • ABI • PT-AFFECTIVE AND/OR ADJUSTMENT ISSUES • PRE-EXISTING AFFECTIVE ISSUES • AGGRAVATION OF PRE-EXISTING CHARACTEROLOGICAL TRAIT AND/OR AFFECTIVE DISORDER • PT-MEDICAL ISSUES • UNRELATED MEDICAL ISSUES • DRUG RELATED SIDE-EFFECTS • DISSIMULATED
STRESS AND IMPACT ON COGNITION & BEHAVIOR • PHYSIOLOGIC EFFECTS • NEUROHORMONAL AND NEUROTRANSMITER CHANGES • PSYCHOLOGICAL EFFECTS • NEGATIVE INFLUENCES ON ATTENTION, CONCENTRATION AND FRUSTRATION TOLERANCE • PATHOANATOMICAL EFFECTS • SUBCORTICAL/HIPPOCAMPAL ATROPHY
SPECIFIC BEHAVIORAL IMPAIRMENTS • FATIGUE/HYPOAROUSAL • HYPERSOMNOLENCE • LIBIDINAL ALTERATIONS • APATHY/ABULIA/LACK OF INITIATION • DYSPHORIA AND DEPRESSION • ANXIETY SPECTRUM DISORDERS INCLUDING PHOBIAS AND PTSD
SPECIFIC BEHAVIORAL IMPAIRMENTS • IRRITABILITY/AGGRESSION • EMOTIONAL LABILITY • OCD • PARANOIA/PSYCHOSIS • MANIA • BPD
TBI and Psychiatric DisordersFrom van Reekum et al. Can traumatic brain injury cause psychiatric disorders? J Neuropsychiatry 12:316-327, 2000
FATIGUE • MOST COMMON CAUSES ARE AFFECTIVE ISSUES AND POOR SLEEP • NEUROGENIC FATIGUE IS A DIAGNOSIS OF EXCLUSION • NEUROMEDICAL ISSUES INCLUDING CHRONIC PAIN CAN PRESENT WITH DEPRESSION • IF DRUGS USED, HAVE ADEQUATE MEASURE PRE- AND POST-TREATMENT AND CORROBORATE PATIENT REPORT AS POSSIBLE • PSYCHOSTIMULANTS ARE NOT THE ONLY DRUGS THAT WORK FOR FATIGUE, CONSIDER NON-CONTROLLED AGENTS FIRST
HYPOAROUSAL AND HYPERSOMNOLENCE • MAY BE RELATED TO SLEEP PROBLEM, UNDERSTIMULATION/BOREDOM, MEDICAL CONDITION, MEDICATION SIDE-EFFECT OR LOW LEVEL NEUROLOGIC STATE • TREAT WHAT CAN BE TREATED FIRST THEN CONSIDER MEDS • DIMS VS. DOES: TX. IMPLICATIONS • SLEEP HYGIENE AND PSGs • DEPENDING ON PRESENTATION, CONSIDER DA AGONISTS AND/OR PSYCHOSTIMULANTS
LIBIDINAL ALTERATIONS • TRUE HYPERSEXUALITY IS UNCOMMON (E.G. KBS) • TREATMENTS INCLUDE BM AND/OR MEDS (HORMONAL OR SEROTONERGIC). IF KBS MAY RESPOND TO AED. • DECREASED LIBIDO • CHECK HORMONES FIRST • GET GOOD HISTORY & R/O DRUG SIDE-EFFECTS • CONSIDER BEHAVIORAL THERAPIES • CONSIDER DRUG TREATMENT - NORADRENERGIC AGENTS, TESTOSTERONE SUPPLEMENTATION
DYSPHORIA AND DEPRESSION • APATHY AND ABULIA MAY BE RELATED TO DEPRESSION AND/OR ORGANICALLY CAUSED • DEPRESSION IS SOMETIMES “OVER-DX’D” • FRONTAL BEHAVIORAL SYNDROMES AND DRUG TREATMENT • DEPRESSIVE MOOD DISORDERS AND DRUG TREATMENT • THERE IS NO “MAGIC” DRUG • CHOOSE DRUG BASED ON PATIENT PROFILE • CONSIDER AUGMENTATION IF SUBOPTIMAL RESPONSE • IF ACUTELY DEPRESSED CONSIDER METHYLPHENIDATE
ANXIETY SPECTRUM DISORDERS • ASDs ARE MORE COMMON IN PERSONS WITH TBI THAN GENERALLY ACKNOWLEDGED • SUB-SYNDROMAL PTSD IS NOT UNCOMMON AND SYNDROMAL PTSD IS SOMETIMES MISSED • MTBI AT TIMES DX’D INSTEAD OF PTSD • THINK ABOUT ASD IN MTBIs WHO ARE NOT GETTING BETTER • CHRONIC PAIN PROMULGATES ASDs • GOOD TREATMENT COMBINES BEHAVIORAL MEDICINE AND PHARMACOTHERAPEUTICS
IRRITABILITY AND AGGRESSION • IRRITABILITY VERY COMMON FOLLOWING TBI • TRUE PHYSICAL AGGRESSION NOT PARTICULARLY COMMON IN POST-ACUTE PHASE • GENERALLY, THIS BEHAVIORAL CLASS OF IMPAIRMENTS RESPONDS WELL TO SSRIs AND/OR PSYCHOTROPIC ANTICONVULSANTS