Download
1 / 29
420 likes | 1.31k Views
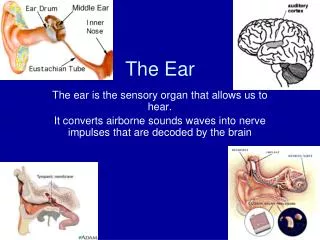
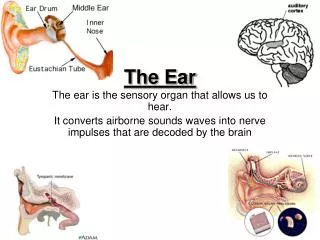
THE EAR. External Ear. Pinna. Tympanic membrane. External Auditory Canal. Pinna /Auricle. Location : oval-shaped appendage on the lateral surface of the head. Auricle elastic cartilage+skin Ear lobule no cartilage (fat and subbutaneous tissue)

E N D
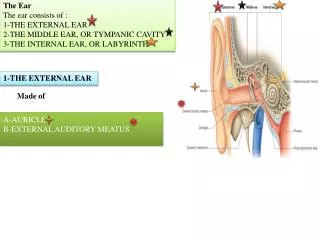
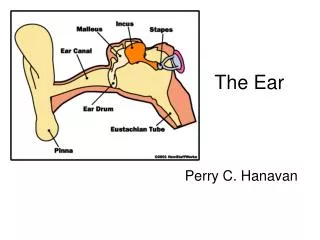
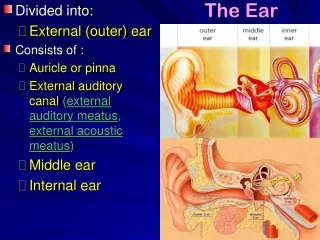
External Ear Pinna Tympanic membrane External Auditory Canal
Pinna/Auricle Location: oval-shaped appendage on the lateral surface of the head. Auricleelasticcartilage+skin Ear lobulenocartilage (fat and subbutaneous tissue) Function: sound localization and amplification. Composition: -thin skin with hair follicles - sweat glands and sebaceous glands covers supporting structure of elastic cartilage
Perichiondritis Definition: • An acute inflammation of the skin and the perichondrium that involves the articular cartilage • Most commonly due to bacterial infection stemming from a small injury in the conchal cavity or the auricle. (close attachment of the skin to the perichondrium) • Causative organisms: staphylococci, pseudomas
Symptoms - Severe pain (rapid onset) - Feeling of tension - Auricular contours are effaced - Swelling of the concha with marked tenderness - Earlobes are spared - Regional lymph nodes maybe painful and enlarged - Fever may occur Treatment • Systemic antibiotics • Cleaning of the auricle and ear canal • Antiseptic/antibiotic containing ointments • Oral analgesics for pain
Trauma EAR TRAUMA
Ear Trauma • Auricle- skin-covered cartilage, with only a thin padding of connective tissue. • The entire cartilage framework is fed by a thin covering membrane called the perichondrium (meaning literally: around the cartilage) • Accumulation of fluid (swelling) or blood (injury) between the perichondrium and the underlying cartilage puts the cartilage in danger of being separated from its supply of nutrients Ear deformity (lumpy, distorted)
Wrestler's Ear (cauliflower ear)- repeated trauma causing thickened auricle that resembles a vegetable. • wrestling is one of the most common ways such an injury occurs. • Ear lobe- devoid of cartilage, covered with adipose tissue.Instead, it is a wedge of adipose tissue covered by skin. • Tears of the earlobe can be generally repaired with good results. Since there is no cartilage, there is not the risk of deformity from a blood clot or pressure injury to the ear lobe. • Other injuries causing major deformity. • Lacerations,bite injuries, avulsion injuries, cancer, frostbite, and burns
External Auditory canal • S-shaped, approx 2.5 cm long • Outer 1/3 cartilage , hair, cilia, mucus, sebaceous glands, ceruminousgland (secretes a brown-like substance, wax-like cerumen “ear wax”) • Inner 2/3 bone (tympanic and squamous portion of temporal bone) , anteroposteriorly , only epithelial lining on the periostium • Skin is very thin, directly overlying the periosteum temperature and pain sensitivity.
The ear's self-cleaning mechanism moves old skin cells and cerumen to the outer part of the ear. • Epithelial migration of the lining of the EAC is a well-known phenomenon and is essential for the self-cleansing mechanism of this structure. • In most cases, the epicenter of this migratory process appears to reside in the vicinity of the umbo of the tympanic membrane. • The epithelial migration takes place at a rate of approximately 0.07mm/day and serves to cleanse the canal of debris, foreign bodies, and bacteria.
Cerumen and Cerumen impaction Cerumen - forms a protective film in which the fatty acids, lysozymes and the creation of an acid milieu bacteriostatic and bactericidal) effectively protects the skin of the ear canal. - Consists of a combination of desquamated epithelium, thick sebaceous gland secretions, and thinner apocrine gland secretions - Water resistant, traps debris
Cerumen impaction - Disturbance of the normal self cleaning mechanism or excessive cerumen secretion.Cerumen plug - Sebum, exfoliative debris, contaminants Symptoms: - pressure sensation in the ear, concomitant hearing loss, occasional vertigo and tinnitus
Cerumenolytics • Ceruminolytics – “cerumen softeners” • Hydrogen peroxide • Mineral oil, baby oil • Commercially prepared otic drops (Otosol, Auralgan) • Water
Foreign Body • Classification • Animate (living) • Bugs • Mosquito • Cockroach • Lice/mites • Inanimate (non-living) • Cotton • Pebbles • Small marbles
Foreign Body: treatment • Methods of removal of foreign body from the ear: • Hooking out - care is taken not to push the foreign body deeper into the ear canal or through the tympanic membrane. • Syringing • Removal under the microscope
Otitisexterna Definition: • Inflammation of the external auditory canal caused by factors that interfere with the normal defenses against infection. Barriers to infection: • Normal cerumen film (acidic pH, fatty acid content- antibacterial) • Lateral migration of the epithelium Predisposing factors: • Exogenous factors - Water (maceration), shampoos (alteration in pH), manipulations with cotton-tipped (overcleaning/daily) swabs, earphones/plugs • Endogenous factors - eczema, allergies, metabolic disorders • Local changes - exostoses, stenoses
S/Sx: • Tragal tenderness • Pain and itching of the ear canal • Erythema • Edema • Canal debris, discharge • Treatment: • Instructions for prevention • Appropriate canal cleaning • Antibiotics • Pain control (analgesics)
Tympanic Membrane • Separates the outer ear from the middle ear. • Consists of 2 portions: pars tensa, pars flaccida • 3 layers of the pars tensa: • Outer- cutaneous layer; smooth muscle, stratified squamous epithelium that reflects the light • Middle- lamina propria; with 2 layers of connective tissue fibers. Outer (radiate layer), inner (circular layer) • Inner- mucosal layer; single layer of squamous epithelium
Pars Flaccida(Sharpnell membrane) • Superior to the malleolar folds • It lacks the reinforcing fibrous layer present in the pars tensa---retracts first in response to negative pressure in the middle ear epithelial pocket
Myringitis • Inflammation of the tympanic membrane • Characterized by: • inflammation • Hemorrhage • Effusion of fluid into the tissue at the end of the external car canal and the tympanic membrane. • This self-limiting disorder (resolving spontaneously within 3 days to 2 weeks) often follows acute otitis media or upper respiratory tract infection and frequently occurs epidemically in children. Bullousmyringitis
Causes: • Viral infection • Bacteria (pneumococci, Haemophilusinfluenzae, betahemolytic streptococci, staphylococci) • organism that may cause acute otitis media. • Symptoms: - severe ear pain - tenderness over the mastoid process - Small, reddened, inflamed blebs form in the canal, on the tympanic membrane - Fever and hearing loss are rare unless fluid accumulates in the middle ear or a large bleb totally obstructs the external auditory meatus. -Bloody discharge- with ruptured blebs - No hearing impairment
Treatment: • Self-limiting • Analgesics • Topical antibiotics- prevent secondary infection
Granular Myringitis • Localized chronic inflammation of pars tensa with granulation tissue • Sequalae of primary acute myringitis, previous otitisexterna, perforated TM • Common organisms: Pseudomonas • Proteus • s/sx: • Foul smelling discharge • Often asymptomatic • No hearing loss/significant pain • No TM perforations • “peeping granulations” • TM obscured by pus
Treatment: • Careful and frequent debridement • Topical anti-pseudomonal antibiotics • Steroids • 2 weeks of therapy
Bulging Tympanic membrane • Bulging tympanic membrane: bulging tympanic membrane occurs due to fluid collection in the middle ear cavity. Causes: - Acute otitis media - Serouseffusion - Glue ear - Tumors Total bulging - a convex-appearing tympanic membrane with loss of visualization of the lateral process and/or the manubrium of the malleus bone. - diagonal cleft in the bulging tympanic membrane where its fibers are tightly adherent to the handle of the malleus. Partial bulging - fullness of an opacified, convex tympanic membrane with preservation of the outline of either the manubrium or the lateral process of the malleus bone. - Mobility is impaired during negative and positive pressure.