Download
1 / 23
340 likes | 1.53k Views
Post-script. Percutaneous mitral valve repair using the MitraClip® device (e-valve). Angela Hoye , Rajesh Nair, Farqad Alamgir Castle Hill Hospital, Hull. No conflict of interest in relation to this presentation. Mitral regurgitation occurs due to: valvular degeneration (50%)

E N D
Post-script Percutaneous mitral valve repair using the MitraClip® device (e-valve) • Angela Hoye,Rajesh Nair, Farqad Alamgir • Castle Hill Hospital, Hull
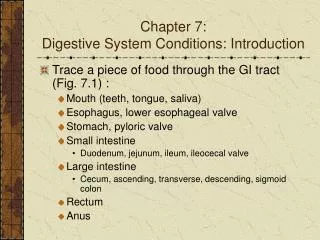
Mitral regurgitation occurs due to: valvular degeneration (50%) rheumatic disease (20%) ischaemia (17%) Where possible, surgical mortality is lower following MV repair rather than replacement However, after MV repair surgery, published data show a rate of recurrence of grade 3 or 4 MR of 17-20% at 5 yrs Introduction: MR
The surgical “edge-to-edge” technique was first described in early 1990`s (Alfieri) Over 1,500 pts reported in the literature Safe, effective, durable No occurrence of mitral stenosis Facilitates proper leaflet coaptation Degenerative - anchor flail / prolapsing leaflets Functional - Coapt tethered leaflets to reduce time and force required to close valve Creates tissue bridge The Alfieri technique
The Alfieri technique • Euro Heart Survey demonstrated that despite presence of severe MR and symptoms, HALF of all patients are not considered for surgery • CE Mark approval in March 2008
Sufficient leaflet tissue for mechanical coaptation Non-rheumatic/endocarditic valve morphology Anatomic considerations Flail gap <10mm Flail width <15mm Mitral Area > 4.0cm Coaptation length > 2mm >2mm >11mm <10mm <15mm Anatomic SuitabilityLeaflet mal-coaptation resulting in MR
Studies • 47 sites
Age 18 years or older Moderate to severe (3+) or severe (4+) MR Symptomatic Asymptomatic with LVEF < 60% or LVESD > 40mm* MR originates from A2-P2 mal-coaptation Candidate for mitral valve surgery Key exclusions: EF < 25% or LVESD > 55 mm Renal insufficiency Endocarditis, rheumatic heart disease Data: EVEREST *ACC/AHA Guidelines, Circ. 114;450,2006
EVEREST I + roll-in phase of EVEREST II Results One or more Clips implanted in 90% of cases
Clinical results 99% 97% Survival 96% 96% 96% 92% 89% Freedom from surgery 86% 85% 82% 84% 75% 67% 66% 65% 63% Freedom from death, surgery & MR > 2+
LV Dysfunction Population (EF < 55% or LVIDs > 4.5cm) Reverse LV remodelling
All potential patients were discussed at MDT Pre-procedural TTE and TOE to determine suitability Teamwork is vital Interventional cardiologist Cardiac anaesthetist ECHO specialist Lab staff – specialist training given to nursing staff All procedures performed with support from physicians from the company Our experience
Successfully treated 3 patients, all with degenerative MR 2 pts with a single clip, 1 with 2 clips No procedural MACE At 1 month, all patients report a marked improvement in symptoms / exercise capacity Our experience
Amplatz Guide
Preliminary results of percutaneous mitral valve repair with the MitraClip® demonstrate that it is safe and feasible Steep learning curve and it is essential to understand MV anatomy and TOE images Definite place for this technology in a subset of patients with MR and suitable anatomy All potential candidates should be evaluated by a multidisciplinary team Patient selection is paramount Conclusions