Download
1 / 17
180 likes | 546 Views
Overview of Methotrexate Clinical Evaluations. Malcolm Smith, MD, PhD Cancer Therapy Evaluation Program National Cancer Institute FDA Pediatric ODAC Meeting - March 2006. 50 Years of Randomized Trials Evaluating Methotrexate for ALL . Acute Leukemia Group B trial

E N D
Overview of Methotrexate Clinical Evaluations Malcolm Smith, MD, PhD Cancer Therapy Evaluation Program National Cancer Institute FDA Pediatric ODAC Meeting - March 2006
50 Years of Randomized Trials Evaluating Methotrexate for ALL • Acute Leukemia Group B trial • Remission induction with prednisolone and vincristine, followed by randomization. • Comparison of 3 mg/m2 daily oral MTX versus 30 mg/m2 twice-weekly IV MTX • Median CR duration: 17 months versus 3 months favoring IV MTX • 50 years later still trying to learn how to use methotrexate JAMA 194: 187-193, 1965
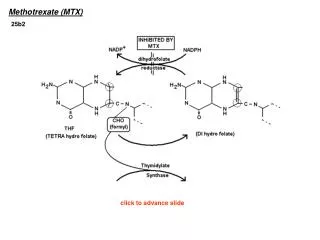
Complexities of Studying Methotrexate • Standardizing high-dose methotrexate? • 1 gm/m2 over 24 hours (POG), • 2 gm/m2 over 24 hours (Dutch) • 5 gm/m2 over 24 hours (BFM) • 8 gm/m2 over 24 hours (NOPHO) • Optimal timing of leucovorin rescue? • 36 hours? 42 hours? 48 hours? • Number of courses of high-dose methotrexate (from 1 to 12)? • Capizzi escalating dose methotrexate and role of asparaginase “rescue”?
Childhood ALL Collaborative Group Overview – Methotrexate Efficacy • Meta-analysis: 8 randomized trials asking an IV MTX (+/-) question of therapy • MTX doses from 0.5 gm/m2 to 8 gm/m2 • Addition of IV MTX to long-term IT therapy or radiotherapy with IT therapy reduced event rate by 17% • IV MTX reduced non-CNS relapse rate • No effect of IV MTX on CNS relapses Clarke, et al. J Clin Oncol 21:1798-1809. 2003
Childhood ALL Collaborative Group Overview – IV Methotrexate Efficacy Clarke, et al. J Clin Oncol 21:1798-1809. 2003
Recent Methotrexate Randomized Studies – POG-9005 • B-precursor ALL – Standard risk • IV MTX 1.0 gm/m2 versus PO MTX 30 mg/m2 every 6 hours for six doses • CCR rate superior for IV MTX compared to PO MTX (p=0.013) • Caveat: Too much leucovorin in the PO MTX arm?? Mahoney, et al., J Clin Oncol, 16: 246-254, 1998
Recent Methotrexate Randomized Studies – POG-9404 • T-cell ALL & lymphoblastic lymphoma • Addition of IV MTX 5.0 gm/m2 to consolidation therapy • 3 EFS (SE) of 72.2% (SE 6.7%) vs. 86.0% (SE 5.6%) for the No HD-MTX and HD-MTX groups • Primary difference in arms for CNS events • Caveat: Delay of radiation in no HD-MTX arm may have increased CNS event rate for control patients Asselin, et al. Proc Am Soc Clin Oncol 20, Abstr #1464. 2001
Recent Methotrexate Randomized Studies – CCG-1882 & CCG-1961 • Evaluated “Capizzi methotrexate” during “interim maintenance” as per “augmented” BFM regimen: • MTX escalating from 100 mg/m2 q 10 days x 5 • Asparaginase 24 hours after MTX • Vincristine q 10 days x 5 • CCG-1882: Improved outcome for SER patients with augmented BFM compared to standard interim maintenance • CCG-1961: Improved outcome for the “augmented” strategy with RER patients • Caveat: Augmented BFM differs from standard COG BFM in ways other than “Capizzi methotrexate”. Nachman, et al., N.Engl.J.Med., 338: 1663-1671, 1998 Seibel, et al. Blood 102 (11), Abstr #787, 2003
Recent Methotrexate Randomized Studies – EFS for CCG-1961 Log rank p = .01 5 Yr EFSRHR Augmented BFM 80.5% Baseline Standard BFM 70.7% 1.42 Years Followed Seibel, et al. Blood 102 (11), Abstr #787, 2003
The Question of the Day • In 2006, what is the best way to administer MTX during the post-remission, pre-maintenance phase of therapy????
Standard ALL Treatment Schema • 8 week treatment block: • Capizzi MTX: • IV 100 mg/m2 MTX q10d x 5 • VCR q10d x 5 • PEG-Asparaginase x 2 • High-dose Methotrexate • 5 gm/m2 MTX x 4 • VCR X 4 • 6MP x 56 days
ALL0232 for High-Risk B-Precursor ALL • 2 x 2 factorial design using an augmented intensity BFM backbone. • Activated December, 2003 • Approximately 2000 randomized patients to enroll in 4+ years of accrual • Randomization 1: Dexamethasone 10 mg/m2/d x 14 days versus prednisone 60 mg/m2/d x 28 days during Induction • Randomization 2: HD-MTX (5 gm/m2) block versus Capizzi escalating methotrexate block during Interim Maintenance I.
ALL0434 for T-cell ALL • 2 x 2 factorial design using an augmented intensity BFM backbone. • To be activated in 2nd Quarter 2006 • Approximately 1200 randomized patients to enroll in 6 years of accrual • Randomization 1: +/- nelarabine during the Consolidation, Delayed Intensification and Maintenance phases of therapy. • Randomization 2: HD-MTX (5 gm/m2) blocks versus Capizzi escalating methotrexate blocks during Interim Maintenance I.
Potential Mediators of Methotrexate-Associated Neurotoxicity Vezmar, et al. Chemotherapy, 49: 92-104, 2003
Methotrexate Neurological Toxicity • Acute neurological toxicity (e.g., seizure) with HD-MTX • Acute neurological toxicity can also be observed with low-dose oral MTX (Winick, et al. JNCI, 84: 252-256, 1992 ) • Chronic neurological toxicity severity ranges from severe leukoencephalopathy to subtle findings on neuropsychological testing • With BPCA support, evaluation of neurological toxicity to become an important secondary objective of both AALL0232 and ALL0434
Summary • Despite more than 50 years of evaluation and treatment refinements, important questions remain to be addressed about how best to use methotrexate for children with ALL. • Future use of methotrexate should be based on data from phase 3 trials evaluating both efficacy and neuropsychological endpoints.