Download
1 / 50
510 likes | 1.01k Views
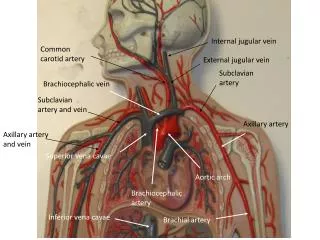
Aortic arch anomalies. Dr.Deepak Raju. Embryology . Heart is first seen in the form of two endothelial heart tubes-18 th day of foetal life Fusion results in a single tube with a series of dilatations(sinus venosus ,atrium ,ventricle & bulbus cordis ) and begins to beat by 22 nd day

E N D
Aortic arch anomalies Dr.DeepakRaju
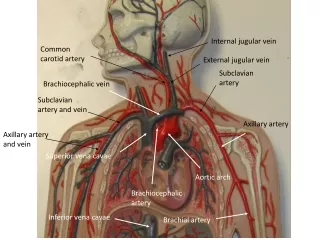
Embryology • Heart is first seen in the form of two endothelial heart tubes-18th day of foetal life • Fusion results in a single tube with a series of dilatations(sinus venosus ,atrium ,ventricle &bulbuscordis) and begins to beat by 22nd day • Bulbuscordis represents arterial end of the tube-prox part conus,distaltruncusarteriosus • First arteries to appear are right and left primitive aorta connected to the endothelial heart tubes • Portion lying ventral to foregut(ventral aorta)-connected to first pharyngeal arch-to the portion dorsal to foregut(dorsal aorta)
After the fusion of endocardial heart tubes,ventral aorta fuse to form aortic sac • Truncus continues with the aortic sac from which right and left pharyngeal arch arteries arises • They arch backward on lateral side of foregut –continues as right and left dorsal aorta-fuse to form descending aorta • During 4th and 5thweek,successive arterial arches appear in 2nd to 6th pharyngeal arches • Each connects ventrally to aortic sac&dorsally to dorsal aorta
Greater part of 1st &2nd arch arteries disappear.1st arch remnant-maxillary artery,2nd arch remnant –hyoid and stapedial artery • 5th arch artery regress completely • 3rd and 4th open to ventral part of aortic sac.6th to dorsal part. • Spiral septum formed in truncus in the 5th week extends to aortic sac.blood from pul.artery goes to 6th arch artery,from aorta to 3rd &4th arch arteries. • Dorsal aorta gives lateral intersegmental branches to body wall.7th cervical intersegmental supplies upper limb bud.
Portion of dorsal aorta b/w 3rd and 4th (ductuscaroticus)disappear • Each 6th arch artery connects to the pulmonary vascular tree.portion b/w this connection and dorsal aorta-ductusarteriosus-regresses on right side
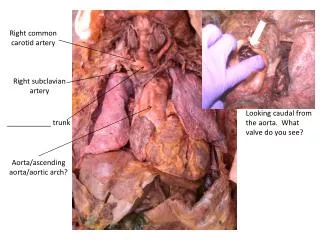
3rd-common carotid and prox.int.carotid • 4th – • Lt.-aortic arch b/w LCCA and LSCA. • Rt-prox RSCA • 6TH – • prox part –proxpul art • distal part-ductus on left and right side involutes • Lt dorsal aorta-aortic arch distal to LSCA • Rt dorsal aorta- • cranial portion-RSCA distal to 4th arch. • distal portion-involutes
Edward s double aortic arch model • Anomalies of aortic arch to be conceptualised as variations in regression of different segments from the hypothetical double arch
History Anomalous RSCA-Hunauld,1735 Double aortic arch-Hommel 1737 Right aortic arch –Fioratti,Aglieti-1763 Interrupted aortic arch-Steidele-1788 Bayford,1787-dysphagia by vasc ring-coined term dysphagialusoria Gross,1945-first division of a vasc ring
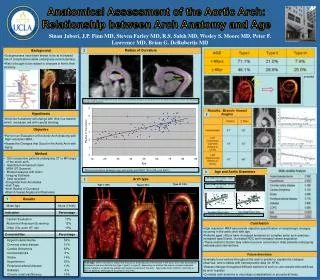
Sidedness of the arch • Left and right arch refers to which bronchus is crossed by the arch • Echo or angio-branching pattern of brachiocephalic vessels • First arch vessel that contains carotid artery opposite side of arch • Retroesophageal or isolated vessels-opp to side of arch • MRI and CT-conclusive
Anatomical classification • Abnormalities of branching • Abnormalites of arch position-cervical arch,right arch • Supernumary arches-double aortic arch and persistent 5th arch • IAA • Anomalous origin of pulmonary artery branch
Clinical classification • Vascular rings • Non-ring vasc.compression • Non-compressive arch malformations • Ductal dependent arch anomalies
vascular ring-aortic arch anomaly in which trachea and esophagus surrounded by vasc. structures Double aortic arch most common(40%),rt.aortic arch with lt.ligamentum(30%),aberrant RSCA(20%),anomalous innominate(10%).
Symptoms- • Stridor,Pneumonia,bronchitis • Reflex apnoea or choking on eating • Hyperextension of neck • Increased resp distress a/wintercurrentresp.infections • swallowing difficulty
3 d΄s opposite to side of arch-diverticulum,dimple,descending aorta • Diverticulum –large vessel from desc.aorta giving rise to a smaller calibre vessel with a sudden taper • Dimple –tapered blindly ending outpouching • Descending aorta in upper thorax opp.to side of arch-connected by ligamentumarteriosum
Variants of left aortic arch • Common brachiocephalic trunk • Right innominate and left carotid from single origin • 10% of normal • Compression of trachea possible • Separate origin of left vertebral artery • 10% • Prox to LSCA • 3rd arch vessel smaller than 4th
Lt arch with retroesophageal RSCA • 0.5% incidence • m.c.arch anomaly • 38% of down′s • Disappearance of Rt 4th arch-distal Rt dorsal aorta becomes prox RSCA • Rt 6th arch disappear • Usually asymtomatic • Barium –smaller filling defect on postr aspect of esophagus slanting upward • Angio-earlier filling of Rt carotid on aortic root injection
Lt ao.arch and retroesophagealdiverticulum of Kommerell • First vasc ring to be diagnosed during life • Similar to previous except for persistent 6th arch-ligamentum which completes a vasc . Ring • Prox.RSCA dilated to form diverticulum
Lt ao.arch,rt.descaorta,rt.ductus(circumflex aortic arch) • Branching pattern similar to earlier-arch retroesophageal,RSCA the last arch vessel is not retroesophageal • Desc.aorta connected to RPA by ligamentum-forms vasc.ring
Lt ao arch &isolated RSCA • Right 6th arch persists • RSCA from rtductus • RSCA and vertebral fills from PA in foetal life • When ductus closes-retrogradely from circle of willis • Vertebrobasilar insufficiency • Congenital subclavian steal • Absent rt arm pulse
Lt ao arch with cervical origin of Rtsubclavian • Marker of 22q11 deletion • Innominate trifurcates in the neck-RSCA travels back to thorax • Subclavian origin from 3rd arch
Right aortic arch • A single aortic arch that crosses rtmainstem bronchus • 13-34% in TOF • 30-40% in truncusarteriosus • 20% in pul.atresia with VSD • 7.7% in tricuspid atresia • 8-10% in transposition
Right aortic arch-mirror image type • Sequence of arch vessels-lt.innominate,rtcarotid,RSCA • Ligamentumlt sided • No vascring.can form rarely if Lt. ductus from rtdesc aorta • CCHD in 98%(48% TOF)
Rtao arch with retroesophagealdiverticulum of Kommerell • Sequence –ltcarotid,rt carotid ,RSCA,a large retroesophageal vessel( diverticulum) from which LSCA arises • Lt ligamentum completes the ring • Disappearance of Lt 4th arch and persistence of 6th arch
Rt arch with retroesophageal LSCA • Similar to previous one except for the absence of retroesophagealdiverticulum • Ductus is rt sided • No vasc ring • Involution of lt 4th and 6th
Rt arch with Lt desc aorta and Lt ligamentum • Aortic arch itself crosses midline-connects to ltductus to form vasc ring
Cervical aortic arch • Arch found above level of clavicle • Two categories-normal branching pattern or anomalous subclavian artery and vascular ring • 2nd group-devidedacc.to carotid origin(bicarotid trunk or separate origin of ext.&int carotid) • Mechanism- • Failure of normal descent of aortic arch system • Persistence of ductuscaroticus&involution of 4th arch-3rd arch becomes definitive aortic arch with separate origin of ext &int carotid from it
Double aortic arch • Both rt and lt arches present • Persistence of both rt and lt 4th arch which join TA sac to dorsal aorta both of which persist • Only one 6th remain • Rarely a/w other CHD, when present-TOF most common • Both arches can be patent or one hypoplastic or atretic(usu.left) • Form complete vasc.rings • Symmetric origin of 4 arch vessels from respective arches when both patent
Persistent 5th arch • First reported by Van praagh in 1969 • Double lumen aortic arch in which both arches appear on same side of trachea • 2 common sub categories- • Subway vessel beneath normal arch(4th arch)that extend from innominate to take off of LSCA • Double lumen aortic arch with atresia of superior arch with patent inferior arch-common origin of all brachiocephalic vessels from asc.aorta
Interrupted aortic arch • Defined as complete separation of ascending and descending aorta • Celoria and Patton classification(1959) • Type A-interruption distal to SCA that is ipsilateral to 2nd carotid artery • Type B-interruption b/w 2nd carotid and ipsilateralsubclavian • Type C-interruption b/w carotids
Each of the types subcategorised to 3 types • 1.without retroesophageal or isolated subclavian artery • 2.with retroesophagealsubclavian artery • 3. with isolated subclavian artery • Interrupted rt arch seen only in DiGeorge syn. • Type A-aorticopulmonaryseptaldefect,TGA • Type B-m.c,a/w conotruncalanomaly,DiGeorge syn. • Type C-rare
Type A-involution of both dorsal aorta distal to 4tharch,prox to persistent 6th arch • Type b-involution of one 4th arch and one dorsal aorta b/w 4th and 6th • Type C-involution of one limb of truncoaortic sac
Present with acute cardiovasc collapse after closure of ductus • Absence of all limb pulse with strong carotid pulse suggest type B with anomalous subclavian
Anomalous origin of pulmonary artery from ascending aorta • Anomalous pulmonary artery branch arising from ascending aorta in presence of a MPA arising separately • Anomalous RPA- • More common • Embryonic branch pul.artery joins rt side of TA sac,but fails to join MPA before septation • High incidence of aorticopulmonaryseptal defect • Anomalous LPA • a/w TOF in 74% • Embryonic branch pul.artery fails to join TA sac • CCF in infancy f/b early devt of pulmonary vascular disease
Anomalous origin of LPA from RPA • LPA arises from RPA and passes b/w trachea and esophagus-pulmonary artery sling • Tracheal compression-severe resp distress and stridor • Isolated anomaly,rarely a/w TOF • LPA passes beyond trachea before joining TA sac • Anterior indentation on barium swallow
Summary • Aortic arch anomalies and vascular rings can be interpreted on the basis of embryology • With the devt. Of MRI and CT 3-D reconstruction is possible • Intervention required only when symptomatic or when a/w other cardiac anomalies