Download

1 / 74
910 likes | 1.61k Views
Pre-Participation Physical Examination. A Principle Tool for Injury Prevention. What is a PPE?. A tool for injury prevention, used to gather medical information about athletes to ensure that they are ready to participate in sports The athlete’s initial exposure to the sport’s medicine team.

E N D
Pre-Participation Physical Examination A Principle Tool for Injury Prevention
What is a PPE? • A tool for injury prevention, used to gather medical information about athletes to ensure that they are ready to participate in sports • The athlete’s initial exposure to the sport’s medicine team
Principles Governing PPE • Collects medical info about athlete to ensure readiness to participate in a sport • Design of PPE should allow assessment of risk factors & detect any disease &/or injury that might create problems • Each question should be understandable • Ensure instruments used are properly calibrated • Each instrument used in PPE should be valid & reliable
Goals of PPE (Kibler, 1990) • Provide an objective, sport-specific musculoskeletal exam • Obtain (-) information that alters participation • Obtain (+) information to decrease injury potential & increase performance • Provide a reproducible record for comparison in the future • Provide baseline data for sport-specific conditioning
Timing & Frequency of PPE • Timing • Researchers say to perform PPE 4-8 weeks prior to start of season • Allows time to f/u on evals, rehab, etc. • Some say at beginning of season • Some say in the season prior to start (i.e. May/June for fall sports) • Frequency • Beginning of each sport season • Beginning of each year • At new level of competition (high school) • Health history update each year
Personnel • General practice physician • Orthopedist • Cardiologist • Athletic trainer • Exercise physiologist • Psychologist • School nurse • Strength coach
formats of the examination • Mass screening • locker room • Individual exams
HISTORY • chronic medical illnesses, • surgical history • allergies • current medications • groups disagreed on questions related to cardiovascular, • neurologic, musculoskeletal, and weight issues. • Preparticipation Physical Examination Task Force
HEENT eye exam Any differences in pupil size (anisocoria)at baseline visual acuity. An athlete should have corrected vision of 20/40 or better if engaging in collision and contact sports Protective eyewear single eye contraindication to participation boxing and wrestling mouth evidence of bulimic activity and/or tobacco A high, arched palate :Marfan’s syndrome ear ruptured tympanic membrane risk factor for participation in swimming and diving
Cardiovascular PPE? • Risk of sudden death in young athlete: • 1/100,000 • Men>women USA:HCM • Age risk Italy:ARVD • geographical diff. Germany:Myocarditis China:Marfan • Silent cardiovascular abnormalities • Such deaths among athletes are unexpected, dramatic,and often elicit community calls for preventive measures • Beta blockers in sport is limitted • Defibrilator is nessesary
goal • earlyidentification of structural cardiac disease associated withsudden death • reduction of the risk of disease progressionassociated with athletic training and competition.
Etiologies of sudden unexplained cardiac death in children and adolescents.
Recommendations and guidelines • The American Heart Association(AHA) • the BethesdaConference • the Italian Guidelines (COCIS) • European Societyof Cardiology(ESC) • International Olympic Committee(IOC)
AHA Cardiovascular PPE Recommendations • 1st yr at institution/high school: - Comprehensive personal and family history - physical examination by qualified examiner - CV PPE every 2 years after initial screening - During intervening years: history ) • Rewritten in 1998 for collegiate athletes: Each year after initial CV PPE: - history - blood pressure measurement
PPE Cardiovascular tests • The AHA states it is not necessary to recommend the use of highly expensive cardiovascular disease tests such as: electrocardiography, echocardiography or graded exercise testing • HOWEVER, they do not discourage the use of these tests
Personnel of CV PPE • Recommended by AHA: • healthcare worker with medical background to reliably obtain a CV history, perform a physical exam and recognize cardiovascular disease. • preferably a licensed physician • Non-physician healthcare workers must establish a formal certification in cardiovascular examinations
The American Heart Association(AHA) and European Societyof Cardiology recommendations
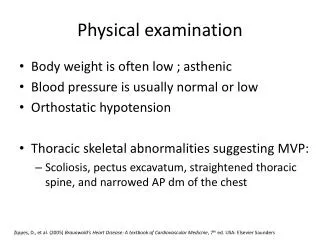
Stigmata of Marfan syndrome • Kyphosis • High arched palate • Pectus excavatum • Arachnodactyly • Arm span > height 1.05:1 or greater • Mitral Valve Prolapse • Aortic Insufficiency • Myopia • Lenticular dislocation
the Italian Guidelines (COCIS) • 12-lead electrocardiogram (ECG) • history • physical examination
investigations • ECG • echocardiography • cardiac magnetic resonance imaging (CMR) • exercise testing • ambulatory Holter ECG recording • implanted loop recorder tilt table examination • electrophysiologic testing with programmed stimulation • Diagnostic myocardial biopsy • genetic testing
CV PPE • ECG • ECG alterations in elite athletes are mostly Twave changes, ST segment elevation, and increases in R and/orS wave voltage • showing ECG abnormalitiesstrongly suggestive of HCM, with diffuse symmetric and pronouncedT wave inversion, associated with increased R or S wave voltagesor deep Q wave • A few others showed ECG patterns suggestiveof ARVC with T wave inversion in V1 to V3 (or V4 • sensitivity 50%, positive predictive value7%
Echocardiography • HCM: • asymmetric left ventricular (LV) wall thickenin • a maximal LV end-diastolic wall thickness of 15 mm or more (or on occasion, 13 or 14 mm) • valvular heart disease (e.g., mitral valve prolapse and aortic valve stenosis) • aortic root dilatation • mitral valve prolapsein Marfan or related syndromes • LV dysfunction and/or enlargement (evident in myocarditis and dilated cardiomyopathy)
some important diseases may escape detection despite expert screening methodology. For example, the HCM phenotype may not be evident when echocardiography is performed in the pre-hypertrophic phase (i.e., a patient less than 14 years of age) • Annual serial echocardiography is recommended in HCM family members throughout adolescence
Athletes with Cardiovascular conditions • referred to a cardiovascular specialist for further evaluation and/or confirmation • refer to 36th Bethesda Conference guidelines • Written in 2005 by American College of Cardiology • Recommendations for determining eligibility for competition in athletes with cardiovascular abnormalities (Maron, 2005)
Judgment of Participation • The American Academy of Pediatrics states: Along with specialist and Bethesda guidelines, should consider: • risks of participation • the advice of knowledgeable experts • current health status • the level of competition, position and sport • availability of effective protective equipment • sport can be modified? • ability of the athlete and parents to understand and accept risks involved in participation
Judgment of Participation • How strenuous the sport is, is another factor that should be considered for athletes with cardiovascular problems • A strenuous sport places many demands on the cardiovascular system
Exercise Stress Test • High Risk Individual • Generally no indication for individual planning mild to moderate exercise
BRUCE PROTOCOL Stage 1 0-3 min 1.7 mph 10% grade 5.0 Mets Stage 2 3-6 min 2.5 mph 12% grade 6.8 Mets Stage 3 6-9 min 3.4 mph 14% grade 9.4 Mets Stage 4 9-12 min 4.2 mph 16% grade 13.3 Mets Stage 5 12-15 min 5.0mph 18% grade 16.6 Mets Stage 6 15-18 min 5.5 mph 20% grade 19.5 Mets Stage 7 18-21 min 6.0 mph 22% grade 22.7 Mets
6 Minute Walk Test • purpose: This test measures aerobic fitness • equipment required: measuring tape to mark out the track distances, stopwatch, chairs positioned for resting. • procedure: The walking course is laid out in a 50 yard (45.72m) rectangular area (dimensions 45 x 5 yards), with cones placed at regular intervals to indicate distance walked. The aim of this test is to walk as quickly as possible for six minutes to cover as much ground as possible. Subjects are set their own pace (a preliminary trail is useful to practice pacing), and are able to stop for a rest if they desire.
6 Minute Walk Test • purpose: This test measures aerobic fitness
Athletic Heart Syndrome • Normal Adaptations to Exercise