Download
1 / 46
562 likes | 1.58k Views
Portal Hypertension. Portal hypertension. Portal hypertension is defined by a portal pressure higher than 5 mm Hg. Type. prehepatic portal hypertension intrahepatic portal hypertension posthepatic portal hypertension. Prehepatic portal hypertension. portal vein thrombosis: the most common

E N D
Portal hypertension • Portal hypertension is defined by a portal pressure higher than 5 mm Hg.
Type • prehepatic portal hypertension • intrahepatic portal hypertension • posthepatic portal hypertension
Prehepatic portal hypertension • portal vein thrombosis: the most common • Infection in the abdominal cavity • omphalophlebitis • A-V fistula between HA and PV
Intrahepatic portal hypertension • Type: • the presinusoidal level • the sinusoidal level • the postsinusoidal level • Cause: • schistosomiasis • hepatitis B and hepatitis C • hepatocellular carcinoma
Postsinusoidal portal hypertension • Cause: • Budd-Chiari syndrome (hepatic vein thrombosis) • constrictive pericarditis • heart failure. • massive splenomegaly (idiopathic portal hypertension) • a splanchnic arteriovenous fistula
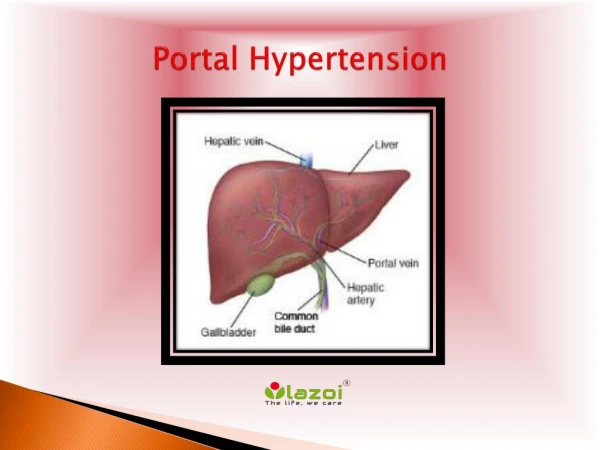
Anatomy of portal hypertension • The portal vein is formed from the confluence of the superior mesenteric inferior mesenteric and splenic veins
Four collateral pathways • Esophageal and gastric venous plexus • umbilical vein from the left portal vein to the epigastric venous system • retroperitoneal collateral vessels • the hemorrhoidal venous plexus
Pathophysiology of portal hypertension • The portal vein contributes two thirds of the total hepatic blood flow • Indirectly regulated by vasoconstriction and vasodilation of the splanchnic arterial bed.
Pathophysiology of portal hypertension portal venous resistance portal venous pressure increase hyperdynamic systemic circulation splanchnic hyperemia portal hypertension collateral pathways established
Clinical manifestation • Upper gastrointestinal hemorrhage • Ascite • Enlarged spleen 、 hypersplenia • Hepatic coma
Laboratory tests • Blood test • Hepatic function: aminotransferase alkaline phosphatase serum bilirubin level • α-fetoprotein level • CT CTA • Magnetic resonance imaging • ultrasound Doppler ultrasonography
Liver Biopsy • A useful technique for establishing the cause of cirrhosis and for assessing activity of the liver disease. • Laparoscopic biopsy
Pressure test • portal pressure can be indirectly estimated by measurement of hepatic venous wedge pressure (HVWP)
Child-Pugh criteria for hepatic functional reserve Clinical and Laboratory Measurement Patient Score for Increasing Abnormality 1 2 3 • Encephalopathy (grade) None 1 or 2 3 or 4 • Ascites None Mild Moderate • Bilirubin (mg/dL) 1–2 2.1–3 ≥3.1 • Albumin (g/dL) ≥3.5 2.8–3.4 ≤2.7 • Prothrombin time (increase, sec) 1–4 4.1–6 ≥6.1 • Grade A, 5 and 6; grade B, 7–9; grade C, 10–15.
Diagnosis • History • Symptom and Physical examination • Laboratory examination Hematology exam CT、CTA USG Endoscopic examination
Treatment • Nonoperative treatments • operative treatments
Nonoperative treatments • Pharmacotherapy • Endoscopic treatment • Balloon Tamponade • Transjugular intrahepatic portosystemic shunt (TIPS)
Pharmacotherapy • Vasopressin: a bolus dose of 20 units over 20 minutes and a continuous infusion of 0.2 to 0.4 unit/minute • Somatostatin is a250-μg intravenous bolus and a continuous infusion of 250 μg/hour for 2 to 4 days • Octreotide :an intravenous bolus of 50 μg and an infusion of 25 to 50 μg/hour for a similar length of time • β-adrenergic blockade
Endoscopic treatment • Sclerosis • Ligation
Balloon Tamponade • Complications esophageal perforation ischemic necrosis of the esophagus
Transjugular intrahepatic portosystemic shunt ( TIPS) • Access is gained to a major intrahepatic portal venous branch through puncture through a hepatic vein. A parenchymal tract between hepatic and portal veins is then created with a balloon catheter,and a 10-mm expandable metal stent is inserted, thereby creating the shunt
Operative treatments • operative mortality rates for Child-Pugh classes A, B, and C • patients are in the range of 0 to 5%, 10% to 15%, and greater than 25%, respectively.
Operative method • a shunt procedure • a nonshunt operation • hepatic transplantation
Nonselective shunts • The end-to-side portacaval shunt • The side-to-side portacaval shunt • The large-diameter interposition shunts • The conventional splenorenal shunt
Selective shunts • the distal splenorenal shunt • the left gastric vena caval shunt • a vein graft between the left gastric (coronary) vein and the inferior vena cava
Partial shunts • a small-diameter interposition portacaval shunt
Nonshunt Operations • esophagogastric devascularization procedures