Download
1 / 5
50 likes | 164 Views
Firewalls, NHS and other organisations’ access to NGS resources Present: Steve Brewer (facilitator/scribe), Gagarine (Greg) Yaikhom, Gareth Smith, David Wallom (towards end to discuss future work). Scenario 1.

E N D
Firewalls, NHS and other organisations’ access to NGS resourcesPresent: Steve Brewer (facilitator/scribe), Gagarine (Greg) Yaikhom, Gareth Smith, David Wallom (towards end to discuss future work)
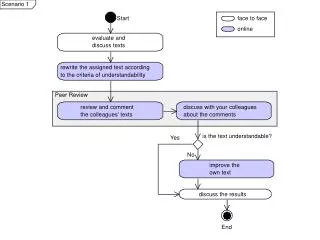
Scenario 1 • Gareth: Shared Genomics Project at Manchester – HPC analysis of large genomic datasets for patients. Providing infrastructure for clinicians and epidemiologists to do statistical analysis of genomic datasets coupled with medical data. (part social science/part bio-informatics). Local cluster with limited no. of users. (note: data already anonymised.) • Wider deployment throughout NHS could benefit a NGS job submission stack eg (RMCS). What will be required? Each deployment will require a liaison person
Scenario 2 • MCTP Monte Carlo Treatment Planning • Currently using Condor at Cardiff and accessing NGS resources at Oxford. • First challenge: clinicians and (perhaps) medical physicists want someone (or something) to sort out account registration and configuration. The tipping point is the language and new technologies (eg SSL) • Second challenge: establishing communication between secure networks such as the NHS and NGS. Default is firewall due to perceived security risk. MofU and/or SLAs needed. Patient data cannot leave the NHS firewall. NHS reluctant to allow the applications inside
Approaches • MCTP: anonymise patient data within NHS firewall, transfer to NGS, return o/p to NHS • Drawback – no standard anonymisation tool for radiotherapy; establishing connection difficult due to use of non-standard ports; conflict of different policy (NHS uses Caldicott rules/guidelines – NHS’s interpretation of data protection law) • Difficult to make progress untill both parties have policy agreements (MoU, SLA etc.) • NHS physicians currently using NGS system to run experiments. Other institutions are acquiring certificates and time – different process – could be streamlined
Future work • NGS is the glue that bridges between institutions. Shiboleth coming. How many NHS institutions are part of the UK Access management Federation. • See SARoNGS (Shibboleth Access to Resources on the National Grid Service )project. • David Wallom to help take forward both scenarios through NGS – solutions proposed • Precedent for MCTP in Genius project at UCL which runs real-time calculations of brain scans for surgeons during procedures. Data is transferred from NGS scanners to NGS and US TeraGrid.