Download
1 / 61
620 likes | 653 Views
BONE. Bone. As a specialized connective tissue Supports fleshly structures Serves as reservoir of Calcium, phosphate and other ions A system of bodily movement Bone cells: Osteoblast Osteocyte Osteoclast Types of bone 1. Compact (Cortical)

E N D
Bone • As a specialized connective tissue • Supports fleshly structures • Serves as reservoir of Calcium, phosphate and other ions • A system of bodily movement • Bone cells: • Osteoblast • Osteocyte • Osteoclast • Types of bone 1. Compact (Cortical) 2. Spongy (trabecular, cancellous, medullary)
Figure 8–3. Events that occur during intramembranous ossification. Osteoblasts are synthesizing collagen, which forms a strand of matrix that traps cells. As this occurs, the osteoblasts gradually differentiate to become osteocytes. The lower part of the drawing shows an osteoblast being trapped in newly formed bone matrix.
Mineralization • Mechanism of mineralization • 1. Collagen fibers • 2. Matrix vesicles • -Produced by osteoblasts and release in matrix • 3.Alkaline phosphatase(ALP) • -in matrix vesicles and osteoblasts membranes • -Matrix vesicles, rich of ALP and other enzymes that involve in rising the concentration of PO4- and promote formation of hydroxyapatite crystals • -Osteocalcin • -Secretes by Osteoblasts • -Non-collagenic polypeptide • -Vit. K dependnet • -Binds to Ca2+ ions and rises its concentration • -Promotes mineralization
Osteocyte -Functions of osteocytes 1- Maintenance of bone matrix 2- Regulation of bone remodeling: - Sclerostin - Special cytokines 3- A broad network of lacunar-canalicular : - Ca2+homeostasis - Detect of mechanical stresses for bone remodeling Fig. 8–4.Osteocytes in lacunae.(a): TEM section of bone showing an osteocyte with its cytoplasmic processes surrounded by matrix. Such processes are extended as osteoid is being secreted and this material calcifies around the processes giving rise to canaliculi in the bony matrix. The ultrastructure of the cell nucleus and cytoplasm is that of a cell no longer active in matrix synthesis.
Osteoclast (Oc) Howship’s lacuna (resorption cavities))
-Two factors secreted by activated osteoblasts for formation and activation of osteoclasts: 1-Macrophage-Colony Stimulating Factor (M-CSF) 2- Receptor Activator of Nuclear k B ligand (RANKL) Figure 8–4. Section showing 3 osteoclasts (arrows) digesting bone tissue. The osteoclast is a large cell with several nuclei and a ruffled border close to the bone matrix. Note the clear compartment where the process of bone erosion occurs. This compartment is acidified by a proton pump localized in the osteoclast membrane. It is the place of decalcification and matrix digestion and can be compared to a giant extracellular lysosome. Chondroclasts found in eroded regions of epiphyseal calcified cartilage are similar in shape to osteoclasts.
Figure 8–5. Bone resorption. Lysosomal enzymes packaged in the Golgi complex and hydrogen ions produced are released into the confined microenvironment created by the attachment between bone matrix and the osteoclast’s peripheral clear zone. The acidification of this confined space facilitates the dissolution of calcium phosphate from bone and is the optimal pH (pH= 4.5)for the activity of lysosomal hydrolases. Bone matrix is thus removed and the products of bone resorption are taken up by the osteoclast’s cytoplasm, probably digested further, and transferred to blood capillaries.
Bone Matrix -Composed of: 50% organic + 50% inorganic 1. Inorganic, Minerals • Hydroxyapatite Crystals: -Calcium & Phosphate (Ca10(PO4)6 (OH)2 ) -superficial ions are hydrtated And forms Hydration shell: Facilitate exchange of ions BTN crystals and body fluids 2. Organic -Collagen type I (90%) -PG + GPs (10%) -PG: Chondroitin sulphate+Keratan sulphate+Hyaluronic acid -GPs: 1.Osteocalcin:Calcium binding protein: increase calcium ion concentration 2.Osteonectin:Ca –and minerals bind to Collagen 3.Sialoproteins:involve in mineralizatoion
Bone Matrix & Mineralization • Mechanism of mineralization • Collagen fibers • 2. Matrix vesicles • -Produced by osteoblasts and release in matrix • 3.Alkaline phosphatase • -in matrix vesicles and osteoblasts membranes • -Suppress of minealization inhibitors such as pyro-organic phosphate (PPI) • -------------------------------------------------- -Composed: 50% organic + 50% inorganic 1. Inorganic, Minerals • Hydroxyapatite Crystals: -Calcium & Phosphate (Ca10(PO4)6 (OH)2 ) -superficial ions are hydrtated And forms Hydration shell: Facilitate exchange of ions BTN crystals and body fluids 2. Organic -Collagen type I (90%) -PG + GPs (10%) -PG: Chondroitin sulphate+Keratan sulphate+Hyaluronic acid -GPs: 1.Osteocalcin:Calcium binding protein 2.Osteonectin:Ca –and minerals bind to Collagen 3.Sialoproteins:involve in mineralizatoion
Figure 8–4.Osteocytes in lacunae. (b): Photomicrograph of bone, not decalcified and sectioned, but dried and ground very thin for demonstration of lacunae and canaliculi, but not cells. The lacunae and canaliculi appear dark and show the communication between these structures through which nutrients derived from blood vessels diffuse and are passed from cell to cell in living bone. X400. Ground bone. Figure 8–2. Photomicrograph of dried bone ground very thin. The lacunae and canaliculi filled with air deflect the light and appear dark, showing the communication between these structures through which nutrients derived from blood vessels flow. Medium magnification.
Periosteum & Endosteum • Periosteum -Sharpey’s fibers (perforating fibers): - Budles of collagen fibers from periosteum that penetrate in matrix and bind periosteum to bone matrix -Outer layer: Dense fibrous layer -Inner layer: Cellular layer 1-Osteoblasts 2-Osteoprogenitor cells: - Appositional Growth & Repair • Endosteum -Osteoprogenitor cell -Osteoblasts -Bone lining cells
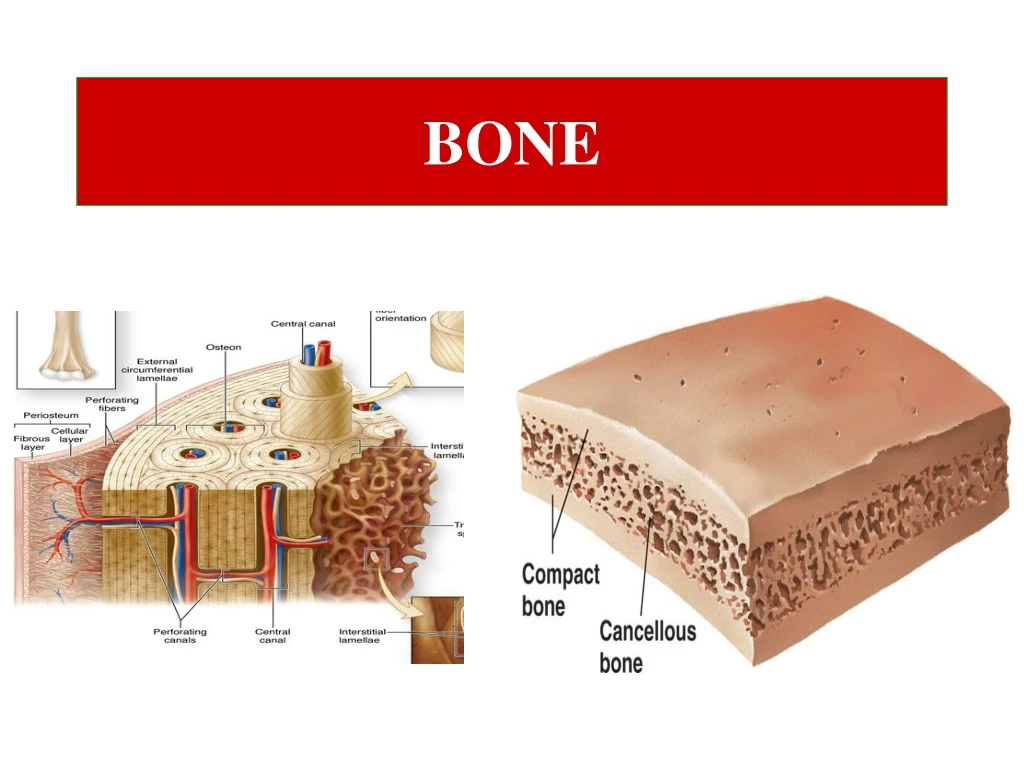
Types of bones • A. Gross observation 1. Compact bone (Cortical) : 80% total volume 2. Spongy bone (Cancellous, Medullary, Trabecular): 20% • B. Appearance morphology • Long bones • Short bones • Flat bones : skull: 2 plates (compact) and Diploe (spongy) • C. Microscopic examination • Primary (immature) bone tissue : Woven bone • Secondary (mature) bone tissue : Lamellar bone
Figure 8–7.Compact and cancellous (spongy or trabecular) bone. Close gross examination of a thick section of dried bone illustrating the cortical compact bone and the lattice of trabeculae in cancellous bone at the bone’s interior. In living tissue the compact bone is covered externally with periosteum and all surfaces of cancellous bone are covered with endosteum.
Microscopic examination • Primary (immature) bone tissue (Woven) a. Temporary, embryonic (Exception: Alveolar bone) b. Irregular array of collagen fibers c. Lower mineral content d. Higher proportion of osteocytes than in secondary bone tissue e. Easily transmission of X-radiation • Secondary bone tissue (Lamellar) a. Collagen fibers arranged in lamellae that are parallel to each other such as haversian system b. Cementing substance: mineralized matrix with few collagen fibers c. Fewer osteocytes between and occasionally within lamellae d. Outer, Inner and interstitial circumferential lamellae
Figure 8–8.Primary (woven) bone. (a): Micrograph of a fractured bone undergoing repair. Primary bone is newly formed, immature bone, rich in osteocytes, with randomly arranged bundles of calcified collagen. Osteoclasts and osteoblasts are numerous in the surrounding endosteum. X200. H&E.
Figure 8–8.Secondary (lamellar) bone.(b): Secondary or mature bone shows matrix organized as lamellae, seen faintly here as concentric lines surrounding osteonic canals. X100. H&E.
Figure 8–6. Schematic drawing of the wall of a long-bone diaphysis showing 3 types of lamellar bone: haversian system and outer and inner circumferential lamellae. (For interstitial lamellae, see Figure 8–10.) The protruding haversian system on the left shows the orientation of collagen fibers in each lamella. At the right is a haversian system showing lamellae, a central blood capillary (there are also small nerves, not shown), and many osteocytes with their processes.
Figure 8–8. Schematic drawing of 2 osteocytes and part of a haversian system. Collagen fibers of contiguous lamellae are sectioned at different angles. Note the numerous canaliculi that permit communication between lacunae and with the haversian canals. Although it is not apparent in this simplified diagram, each lamella consists of multiple parallel arrays of collagen fibers. In adjacent lamellae, the collagen fibers are oriented in different directions. The presence of large numbers of lamellae with differing fiber orientations provides the bone with great strength, despite its light weight.
Figure 8–10.Lamellar bone: Perforating canals and interstitial lamellae.(a): Transverse perforating canals (P) connecting adjacent osteons are shown at the left side of the micrograph. Such canals “perforate” lamellae and provide another source of microvasculature for the central canals of osteons. Among the intact osteons are also found remnants of eroded osteons, seen as irregular interstitial or intermediate lamellae (I). X100. (b): Schematic diagram shows remodeling of compact lamellar bone showing three generations of osteonic haversian systems and their successive contributions to the formation of interstitial lamellae. Remodeling is a continuous process that involves the coordinated activity of osteoblasts and osteoclasts, and is responsible for adaptation of bone to changes in stress, especially during the body’s growth.
Figure 8–10. Schematic drawing of diaphyseal bone remodeling showing 3 generations of haversian systems and their successive contributions to the formation of intermediate, or interstitial, lamellae. Remodeling is a continuous process responsible for bone adaptations, especially during growth.
Figure 8–11.Development of osteons. During remodeling of compact bone, a group of osteoclasts acts as a boring cone (Cutting cone) to make a tunnel into bone matrix. Behind these cells a population of osteoblasts enters the tunnel and lines its walls. As the osteoblasts secrete osteoid in a cyclic manner, they produce layers of new matrix with cells trapped in lacunae (Closing cone) . The cells in lacunae are now osteocytes. The tunnel becomes constricted with multiple concentric layers of new matrix and its lumen finally exists as only a narrow central canal with small blood vessels.
Figure 8–12 Tetracycline localization of new bone matrix. Newly formed bone can be labeled with the molecule tetracycline, which forms fluorescent complexes with calcium at ossification sites and provides an in vivo tracer to localize bone formation. A group of osteons in bone after tetracycline incorporation in vivo seen with bright-field (a) and fluorescent microscopy (b) reveals active ossification in one osteon and the external circumferential lamellae (upper right). .
Histogenesis (Osteogenesis) • Intramembranous ossification • Endochondral ossification
Figure 8–12. The beginning of intramembranous ossification. Mesenchymal cells round up and form a blastema, from which osteoblasts differentiate, producing primary bone tissue.
Figure 8–12.Intramembranous ossification. Developmental process by which most bones of the skull are formed. (a): Groups of mesenchymal cells in a “membrane” or sheet of this embryonic tissue, round up and differentiate as osteoblasts producing osteoid. (b): Cells trapped in the calcifying matrix differentiate as osteocytes. (c): Woven bone is produced in this manner, with vascularized internal spaces that will form the marrow cavity and surrounded on both sides by developing periosteum. (d): Remodeling of the woven bone produces the two layers of compact lamellar bone with cancellous bone in between, which is characteristic of these flat bones.
Figure 8–13. Intramembranous ossification. A section of jaw from a fetal pig undergoing intramembranous ossification. (a): Areas of typical mesenchyme (M), condensed mesenchyme (CM) adjacent to aggregates of new osteoblasts (O). Some osteoblasts have secreted matrices of bone (B) which remain covered by osteoblasts. Between these trabeculae of newly formed primary bone are vascularized areas (V) that will form marrow cavities. X40. H&E. (b): Higher magnification shows the developing periosteum (P) that covers masses primary bone that will soon merge to form a continuous plate of bone. The larger mesenchyme—filled region at the top is the developing marrow cavity. X100. H&E.
Figure 8–14.Osteogenesis of long bones by endochondral ossification. Endochondral ossification forms most bones of the skeleton and occurs in the fetus in models made of hyaline cartilage (1). • The process takes many weeks and major developmental stages include: formation of a bone collar around the middle of the cartilage model and degeneration of the underlying cartilage (2), followed by invasion of the resulting ossification center by capillaries and osteoprogenitor cells from the periosteum(3), osteoid deposition by the new osteoblasts, calcification of woven bone, and its remodeling as compact bone (4). This primary ossification center develops in the diaphysis, along the middle of each developing bone. Secondary ossification centers develop somewhat later by a similar process in the epiphyses. The primary and secondary ossification centers are separated by the epiphyseal plate (5) which provides for continued bone elongation. The two ossification centers do not merge until the epiphyseal plate disappears (6) when full stature is achieved.
Figure 8–13. Formation of a long bone on a model made of cartilage. Hyaline cartilage is stippled; calcified cartilage is black, and bone tissue is indicated by oblique lines. The 5 small drawings in the middle row represent cross sections through the middle regions of the figures shown in the upper row. Note the formation of the bone collar and primary and secondary ossification centers. Epiphyseal fusion with diaphysis, with disappearance of the epiphyseal cartilage, occurs at different times in the same bone.
Figure 8–19. Section of endochondral ossification. The osseous matrix, rich in collagen type I, is specifically stained with picrosirius-hematoxylin. The cartilaginous matrix, containing collagen type II, stains blue with hematoxylin because of its high content of chondroitin sulfate. Medium magnification.
Figure 8–15.Cells and matrices of a primary ossification center. A small region of a primary ossification center showing key features of endochondral ossification. Compressed remnants of calcified cartilage matrix (dark purple), now devoid of chondrocytes, are enclosed by more lightly stained osteoid or bone matrix. This newly formed bone is surrounded by a layer of large, active osteoblasts. Some osteoblasts that were captured by the matrix have become smaller osteocytes (arrowheads). X200. Pararosaniline–toluidine blue.
Epiphyseal cartilage is divided into 5 zones: • Resting zone • Proliferative zone • Hypertrophic zone • Calcified zone • Ossification zone
Figure 8–16.Epiphyseal growth plate: locations and zones of activity. The large and growing primary ossification center in long bone diaphyses and the secondary ossification centers in epiphyses are separated in each developing bone by a plate of cartilage called the epiphyseal plate. (a): Epiphyseal plates can be identified in an x—ray of a child’s hand as marrow regions of lower density between the denser ossification centers. Cells in epiphyseal growth plates are responsible for continued elongation of bones until the body’s full size is reached. Developmental activities in the epiphyseal growth plate occur in overlapping zones with distinct histological appearances. (b): Moving from the epiphysis to the diaphysis, these zones include cells specialized for the following: (1) normally appearing hyaline cartilage, (2) cartilage with proliferating chondroblasts aligned in lacunae as axial aggregates, (3) degenerating cartilage in which the aligned cells are hypertrophic and the matrix condensed, (4) an area in which the chondrocytes have disappeared and the matrix is undergoing calcification, and (5) a zone in which blood vessels and osteoblasts have invaded the lacunae of the old cartilage, producing marrow cavities and osteoid for new bone. X100. H&E.
Figure 8–17.Cells and matrices of the epiphyseal growth plate. • (a): At the top of the micrograph the growth plate (GP) shows its zones of hyaline cartilage with cells undergoing rest (R), proliferation (P), and hypertrophy (H). As the chondrocytes swell and degenerate they release phosphatase, activities which compress the matrix and cause an initial deposition of CaPO4. This produces calcified spicules (C) in the former cartilage matrix. The tunnel—like lacunae in which the chondrocytes have undergone apoptosis are invaded from the diaphysis by large, thin—walled blood vessels which begin to convert these spaces into marrow (M) cavities. Endosteum with osteoblasts also moves in from the diaphyseal primary ossification center and these cells cover the spicules of calcified cartilage and lay down layers of osteoid, forming a supportive matrix that is now largely primary woven bone (B). X40. H&E. • (b): Higher magnification shows more detail of the cells and matrix spicules in the zones undergoing hypertrophy (H) and ossification. Staining properties of the matrix clearly change in this process: first when it is compressed and begins to calcify (C), and then when osteoid and bone (B) are laid down. The large spaces between the ossifying matrix spicules become the marrow cavity (M), in which sinuses of eosinophilic red blood cells and aggregates of basophilic white blood cell precursors can be distinguished. The marrow is the major site of blood cell formation in adults. X100. H&E.
Figure 8–18.Main features of bone fracture repair. Repair of a fractured bone occurs through several stages, but utilizes mechanisms already in place for bone remodeling. • (1): Blood vessels torn within the fracture release blood which clots to produce a large fracture hematoma. • (2): This is gradually removed by macrophages and replaced by a soft fibrocartilage—like mass of procallus tissue rich in collagen and fibroblasts. If broken, the periosteum re—establishes continuity over this tissue. • (3): This soft procallus is invaded by regrowing blood vessels and osteoblasts. In the next few weeks the fibrocartilage is gradually replaced by trabeculae of primary bone, forming a hard callus throughout the original area of fracture. • (4): The primary bone is then remodeled as compact and cancellous bone in continuity with the adjacent uninjured areas and fully functional vasculature is re—established.
Figure 8–21. Repair of a fractured bone by formation of new bone tissue through periosteal and endosteal cell proliferation. Both endochondral and intramembranous ossification processes contributing simultaneously to the healing of fractures.
99% of body Calcium : Calcium storage • Calcium Exchange BTN blood and Bone • Calcium circulating : • Fast : from Hydroxyapatite to interstitial fluid : Spongy bone • Slow: Hormone –dependent • Parathyroid: On osteoblasts: secrete Osteoclast-stimulating factor: Bone absorption by steoclasts :Calcium relaese • Calcitonin: Inhibiting factor on Osteoclast function : inhibition of bone absorption • Diseases: • Hyperparathyroidism: Hyperactivity of osteoclasts: severe absorption of bone, High rate of blood calcium and phosphate ions, • Osteopetrosis: Defect in osteoclast function: bone thickness:Reduce of bone marrow production, Anemia, infection
JOINTS • Classifications: a. Diarthroses: permit free bone movement - Unite long bones and have great mobility : knee joint - b. Synarthroses: very limited or no movement 1. synostosis: bones are united by bones, No movement: Skull bones 2. Synchondrosis: bones joined by cartilage: epiphyseal plate 3. syndesmosis: Dense connective tissue: Skull bones in children