Download
1 / 16
160 likes | 163 Views
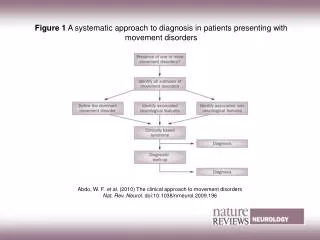
This article provides an overview of the NICE guidelines for managing patients presenting with symptoms of atrial fibrillation, including breathlessness, palpitations, syncope/dizziness, and chest discomfort. It covers topics such as confirming rhythm through ECG and echo, stroke risk assessment, rate control, rhythm control, and stroke prevention therapy. The article also discusses when to consider specialist referral, AF ablation, and cardioversion.

E N D
NICE 2014 Check pulse in patients presenting with: breathlessness/dyspnoea palpitations syncope/dizziness chest discomfort stroke/transient ischaemic attack.
NICE Bullet Points Confirm rhythm – ECG Echo – only if will alter management Stroke risk / bleeding risk assessment If VKA – monitor TTR Rate control is first line Rx Specialist referral: refer people promptly at any stage if treatment fails to control the symptoms of atrial fibrillation and more specialised management is needed. Consider AF ablation if ongoing symptoms (Paroxysmal AF) Consider PPM / Avnodal ablation if ongoing symptoms (Permanent AF)
NICE 2014 Stroke prevention Do not offer stroke prevention therapy to people aged under 65 years with atrial fibrillation and no risk factors other than their sex (that is, very low risk of stroke equating to a CHA2DS2-VASc score of 0 for men or 1 for women). [new 2014] No place for aspirin unless another indication eg IHD
NICE 2014 – Rate vs Rhythm • Offer rate control as the first-line strategy to people with persistent atrial fibrillation, except in people: • Reversible cause • Heart failure caused by atrial fibrillation with new-onset atrial fibrillation • Atrial flutter whose condition is considered suitable for an ablation strategy to restore sinus rhythm • A rhythm control strategy would be more suitable based on clinical judgment
General Management of the AF Patient Secondary care
Conditions predisposing to, or encouraging progression of AF
Initial management of AF • History (including alcohol intake), examination, blood tests, ECG. • Cardiac echo if murmur or very abnormal ECG or no predisposing cause. • Anticoagulant after calculating thromboembolic risk • Rate control agents • Treat any underlying conditions • Refer if severe haemodynamic compromise, poor rate control, complex heart disease or for consideration of cardioversion • Do not need hospital referral if fast AF but not severely compromised.
Rhythm Control vs Rate Control • NICE 2014 – Rate Control • Standard BB or rate control CCB • Dig as mono-RX only if sedentary • Combine agents as required • Do not use amiodarone • If fails – ablate & pace • Rate Control • Beta blockers • Verapamil/Diltiazem • Digoxin • Av V node ablation + Pacemaker
614 Perm AF Strict (rest HR <80) Vs Lenient AF (rest HR <110) 1-EP: CV death / HF admit / CVA / embolism / bleeding / life threatening arrhythmia 45% BB alone 6% CCB alone 7% Dig alone 17% BB + Dig 3% BB + CCB 5% CCB + Dig 1% BB + Dig + CCB 14.9% vs 12.9% at 3-years; NS
Rhythm Control vs Rate Control • Rhythm Control • Cardioversion • Class I Agents (edflecainide) • Beta-blockers • Sotalol Class III Dose • Amiodarone • Direct AF Ablation • - PV Isolation • - LACA • NICE 2014 – Rhythm Control • Continued symptoms despite controlled rate • Recent onset and rhythm control likely to be successful • Amiodarone if bad LV • Amiodarone to consolidate DCCV • 1c-Agent only if normal heart • PVI for PAF if drugs fail
Who to refer for cardioversion? No clear guidelines Symptomatic persistent AF < 12 months with no serious underlying heart disease AF with precipitating cause eg thyrotoxicosis, chest infection now treated Tachycardia induced cardiomyopathy Chances lower with long duration of AF,large LA, mitral valve disease, class III or IV NYHA Not if asymptomatic and age > 60