Download
1 / 19
190 likes | 204 Views
Nutrition and Kidneys. MNT Approaches to Acute and Chronic Kidney Disease. What happens when Kidneys shut down?. Waste products Water/fluids Parathyroid Electrolyte balance The diet of patients with compromised kidney function corrects the chemical imbalances. Key Labs to Watch.

E N D
Nutrition and Kidneys MNT Approaches to Acute and Chronic Kidney Disease
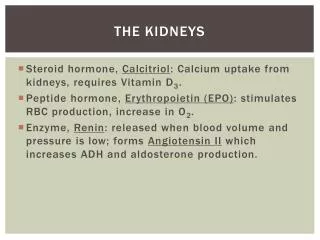
What happens when Kidneys shut down? • Waste products • Water/fluids • Parathyroid • Electrolyte balance • The diet of patients with compromised kidney functioncorrects the chemical imbalances
Key Labs to Watch • BUN/Creatinine • K • Phos • Albumin • Hgb, Hct • Calcium • Body weight changes
Acute Renal Failure • Short term kidney failure • See rapid change in chemistry, water retention • Cause: infection or trauma • Diet Rx: support underlying disease process, keep comfortable, monitor for fluid buildup
Chronic Renal Failure • Slow to occur – gradual onset • Causes: uncontrolled HTN, DM, CA, Lupus, trauma • Symptoms – yellowing of skin, retention of water, weight loss, appetite loss, “don’t feel good” usually brings to Dr OR product of long term monitoring
Diet Rx for CRF (predialysis) • To retard kidney destruction, limit protein to .08g/kg/day. • Sometimes losing too much water and electrolytes – base this on the chemistries
Going on Dialysis Types of treatments • Hemodialysis • In Center • Home • Peritoneal • Continuous (CAPD) • Intermittent (IPD) • Continuous Cyclic (CCPD) • Transplant
Diet for Hemodialysis • 1 gm protein per kg body weight • 2 gm K • 2 gm Na • Limited phosphorus • 1500 cc fluid q d • Kcalories to meet need or control blood glucose
Typical Lab Panels • BUN – look for up to 100 pretx • K - < 6.0 • P - < 6.0 • Alb - > 3.0 • Wt changes – 2-3 kg • Monitor weight trend by post tx when they are “dry”
Medications (lots) • Calcium supplement (phosphate binder • Multivitamin • Iron supplement or antianemics • Antihypertensives (usually) • Control of other conditions eg, CA tx, oral agents, CVD
Pros/Cons of Hemodialysis • Someone else controls tx • Scheduled • Control over cleansing of blood • In center attention and often • But • Fluid buildup • Constant control of external chemicals to prevent buildup • BP drops • Access infections
Peritoneal Dialysis • Continuous exchanges of sugar fluids to remove waste • Goods: feel better, better clearance of chemistries, less restrictive diet • Bads: requires independence, weight gain, difficult protein balance, more difficult to control BGL, high susceptibility to infection of access
Diet Rx for Peritoneal Dialysis • High protein – 2 gm/kg body weight • Calorie controlled • Balanced nutrients • Phosphorus restriction
Meds for Peritoneal patients • Multivitamin • antianemics • Support meds for underlying conditions
Labs for Peritoneal patients • BUN – 40-50 • Albumin > 3.0 • Phos < 6.0 Spend lots of time counseling on balance between adequate protein and just enough kcalories to control weight (additional kcals from dialysate fluid)
Transplant – the end of Kidney Disease? • Symptoms and ramifications of ESRD subside • High doses of antirejection drugs result in weight gain (round face) • Also they feel better, and eat more • Diet Rx: kcalorie controlled, balanced (avoid weird stuff)
Issues with ESRD patients • Noncompliance • Denial • Lose hope • More and more elderly • Family control of diet
What you do when you work with a patient with renal disease • Assess: no question is high acuity level, start as you would anyone else with calculating nutrient needs and adjustment • Plan: continous, they are going to be with you awhile • Educate: ongoing, sometimes fruitless, develop a trust level with your patients • Monitor: look for trends and real changes