Download

1 / 41
530 likes | 1.01k Views
Meningococcal disease. SSU assistant professor Bynda T . P. RELEVANCE OF THE TOPIC. Among infectious diseases, meningococcal disease (MD) is one of the life-threatening and unpredictable for fulminant course. RELEVANCE OF THE TOPIC.

E N D
Meningococcal disease SSU assistant professorBynda T. P.
RELEVANCE OF THE TOPIC • Among infectious diseases, meningococcal disease (MD) is one of the life-threatening and unpredictable for fulminant course.
RELEVANCE OF THE TOPIC • In the world, approximately 500,000 cases of MD are recorded annually, of which about 50,000 are fatal. • Despite the fact that the incidence of meningococcal disease is relatively low compared with other infections, the mortality rate according to world data is approximately 10%. • In Ukraine today, the mortality rate for meningococcal disease reaches 11% -17%. Every year in Ukraine 40 adults and 100 children die from meningococcal disease. • Most of the adverse effects of meningococcal disease is accounted for by meningococcemia.
RELEVANCE OF THE TOPIC • The incidence rate among children is always several times higher than that of adults, reaching 8–11 cases per 100 thousand people. • More than 50% of the total number of cases are children under 5 years old. • It is in children that the frequency of development of generalized forms of MD is high. • To a large extent, the risk of death in MD depends on the age of the child: the younger he is, the higher the probability of an adverse outcome.
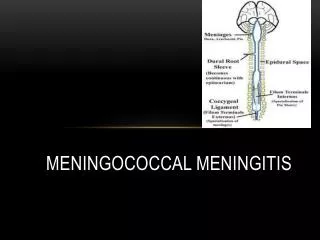
Meningococcal disease Acute anthroponotic infectious disease, caused by the bacteriumNeisseria meningitidis, with drip (aerosol) mechanism of transmission; clinically characterized by lesions of the nasopharyngeal mucosa (nasopharyngitis), generalization in the form of specific septicemia (meningococcemia) and inflammation of the pia mater (meningitis).
ETIOLOGY • Meningococcus by capsular polysaccharide is divided into 12 serogroups: А, В, С, X, Y, Z, W-135, 29E, К, Н, L, I.
ETIOLOGY • More than 20 serotypes and meningococcal subtypes are distinguished by antigens in membrane proteins. • According to lipopolysaccharide immunotypes - more than 11 immunotypes. • The ability of meningococci to form L-forms that are likely to cause prolonged variants of meningitis has been proven.
EPIDEMIOLOGY • Major epidemics in the twentieth century, which simultaneously covered many countries of the world, were caused by meningococcal serogroup A; local epidemic rises within the borders of one country– by meningococcal serogroups B and C; sporadic disease incidence of interepidemic period was mainly formed by serogroupsA, B, C, Y, W-135. • In Ukraine meningococcus of group B prevail.
EPIDEMIOLOGY • The bacterium is transmitted from person to person by airborne and contact routes. • 10-20% of the population are carriers of N. meningitidis. However, in epidemic situations the number of carriers may be higher.In the epidemiological sense, carriers are the most dangerous, as there are 1200–1800 carriers per person
MORBIDITY IN AFRICA • The highest rates of this disease are found in the meningitis belt in sub-Saharan Africa, stretching from Senegal in the west to Ethiopia in the east.
CAUSES OF HIGH MORBIDITY OF CHILDREN • The presence of a protective capsule in meningococcus (as well as that in the Haemophilus influenzae and pneumococci), small children (1-5 years old) are unable to effectively develop immunity against natural infection.The result of this is that the peak of meningitis occurs in younger children..
RISK GROUPS • Children with asplenia or a remote spleen, with sickle cell anemia, with liquorrhea, after surgery for cochlear implantation, as well as with a number of forms of primary immunodeficiency are at particular risk.(deficiency of complement components С5-9).
MENINGOCOCCAL DISEASE OUTCOMES • If untreated, meningococcal infection is fatal in 50% of cases. • But even in cases of early diagnosis and proper treatment, 5-10% of patients die, as a rule, 24-48 hours after the onset of symptoms from intractable acute edema and brain swelling, infectious toxic shock, acute adrenal insufficiency.
Complications after disease • Even in the case of diagnosis and proper treatment in the early stages of the disease there is a high risk of death. • In 10–20% of surviving people, bacterial meningitis can cause brain damage, hearing loss, or learning difficulties.
Complications Of Meningococcal Meningitis epileptiform syndrome hydrocephalus neuroendocrine disorders Paralysis, paresis encephalasthenia Damage of II, VI, VIII exacerbation of chronic infections cranial nerve pyelitis cystitis
PREPARATIONS FOR ACTIVE IMMUNOPROPHYLAXIS Meningococcal vaccines contain purified capsular polysaccharides. Today, there are two types of vaccines against meningococcal disease: • Polysaccharide unconjugated. Unconjugated vaccines are not used to vaccinate children under the age of 2 through their low immunogenicity; • Polysaccharide conjugate vaccines. Conjugation of the polysaccharide antigen makes it possible to ensure the high immunogenicity of the vaccine during vaccination of children under 2 years of age.
POLYSACCHARIDE VACCINES • Polysaccharide unconjugated vaccines cause a fairly strong immune response and give protection for at least 3 years; their epidemiological effectiveness reaches 85–95%. • However, the limitation of their use is the inability to induce a T-cell response in children up to 1.5–2 years old, in whom the meningococcal disease is particularly severe.
POLYSACCHARIDE VACCINES • Meningococcal polysaccharide vaccines intended to control of diseaseare bivalent(groups A and C), trivalent (groups A, C, and W) or tetravalent (groups A, C, Y, and W135).
Vaccines • To develop polysaccharide vaccines against bacteria of group B is impossible due to antigenic mimicry with polysaccharides in human neurological tissues.Therefore, vaccines against group B, used in particular in Cuba, in New Zealand and Norway, were the outer membrane protein (NBM) and were intended to combat epidemics caused by specific strains. Other universal protein vaccines of group B are in the final stages of development.
CONJUGATE VACCINES • Since 1999, meningococcal conjugate vaccines against group C have been available and are widely used. • Since 2005, the quadrivalent conjugate vaccine against groups A, C, Y and W135. • Conjugate vaccines have been licensed for use among children and adults in Europe, Canada and the United States of America.
CONJUGATE VACCINE A new conjugated vaccine against meningococcal group A, introduced in 2010, has a number of advantages over existing polysaccharide vaccines: • it causes a stronger and more stable immune response to meningococcus group A; • reduces the carriage of bacteria in the throat. It is expected that it will provide long-term protection not only for vaccinated people, but also for family members and other people who would otherwise be exposed to meningococcus. The vaccine is available at a lower price compared to other meningococcal vaccines; It is expected to be particularly effective in protecting children under two years of age who do not respond to regular polysaccharide vaccines.
CONJUGATE VACCINE • A conjugated vaccine against meningococcal serotype C, currently prevalent in Europe, has now been developed. • In the UK, this vaccine is included in the National Calendar for vaccinating children from the age of two months.
Vaccines that are included in the national calendars of the United States and European countries • Vaccine meningococcal group A polysaccharide dry, • polysaccharide meningococcal vaccine A + C, • «Menactra», • «Mencevax ACWY», • «Meningo А+С», • «Menugate».
Vaccines http://ilive.com.ua/health/privivka-ot-meningokokkovoy-infekcii_70387i16110.html
Menactra - Conjugated Meningococcal Vaccine • Menactra (Sanofi Pasteur) - the world's first tetravalent meningococcal conjugate vaccine, was developed and licensed in the United States in 2005. From 2005 to 2013, more than 71 million doses of this vaccine were produced. • The use of this vaccine allows you to immunize children in order to form a long-lasting immunity against meningococcal infection. This vaccine targets four of the five most common serotypes A, C, Y, W that cause severe forms of meningococcal disease. • Unlike polysaccharide vaccines, conjugated meningococcal vaccines provide for the formation of immunological memory, i.e. more prolonged protection against meningococcal infections in vaccinated individuals.
Vaccine Mentsevax ACWY company “Glaxo SmithKline” used to vaccinate pilgrims to Mecca, where meningococcal serotypes W and Y circulate.
Polysaccharide meningococcal vaccines types A and C • Polysaccharide meningococcal vaccines types A and C are immunogenic in persons older than 2 years of age and protect against infection for at least 3 years. • Their epidemiological effectiveness reaches 85–95%. • Vaccines are insufficient immunogens for children younger than 2 years old.
VACCINES REGISTERED IN UKRAINE • MENINGO A+C/МЕНІНГО А+С Vaccine for the prevention of meningococcal infection of serogroups A and C polysaccharide, dry (France) (№100/08-300200000)
MENINGO A+C • Meningo A + C - Aventis Pasteur (France) vaccine contains 50 µg of purified lyophilized meningococcal polysaccharides, corresponding to (A, C) serogroups. • Release form: vials of 1, 10, 20, and 50 doses.
MENINGO A+C: Release form Solution for injection, obtained by dissolving the lyophilisatewith solvent. • Lyophilisate: vials containing 1, 10 or 50 doses • Solvent: Syringe containing 1 dose (0.5 ml). Vial containing 10 doses (5 ml). Vial containing 50 doses (25 ml).
MENINGO A+C: Indications in Ukraine • Separate groups of patients with an increased risk of developing an infection and a severe or fulminant form of the course. • To control outbreaks of infection caused by serogroups of microorganisms that are contained in the vaccine. • Adults and children over 2 years of age with functional and anatomical asplenia due to the potential risk of a fulminant course of meningococcemia. If possible, the vaccine should be administered 10-14 days before splenectomy. • With an epidemic increase in the incidence of generalized forms of infection (more than 2.0 per 100 000 population), in the foci of infection caused by the corresponding serogroups of pathogens.
MENINGO A+C: TERMS OF VACCINATION • Vaccination is carried out once, starting at 18 months of age. • The optimal timing of revaccination at the present stage has not been established.
MENINGO A+C:способ введения, схема применения • Растворить лиофилизат с помощью входящего в комплект растворителя. • Вакцина вводится подкожно или внутримышечно. • Разведенная вакцина должна быть использована немедленно. Если вакцина оставлена в шприце, после использования его следует уничтожить. • Лица групп риска, привитые ранее полисахаридной вакциной, могут быть привиты конъюгированной вакциной.
РЕАКТОГЕННОСТЬ ВАКЦИН • Вакцина Менинго А+С мало реактогенна. • Менцевакс АСWY редко вызывает температуру в течение 1 дня, местные реакции – покраснение, болезненность в месте укола. • Вакцина Мenactra также мало реактогенна, повышение температуры до 38 °C после ее введения отмечался у подростков в 5,1% (при введении 4-валентной полисахаридной вакцины – в 3,0%), у взрослых соответственно в 1,5 и 0,5%. Несколько чаще отмечались и местные реакции.
Meningo A + C VACCINE: CONTRAINDICATIONS • Acute infectious diseases. • Progressive diseases in the stage of decompensation (acute or chronic). • The vaccine should not be used in individuals who have previously experienced a severe reaction to the introduction of this vaccine or its component. • Between serogroups of meningococcus cross protective immunity is not formed.
Meningo A + C VACCINE: CONTRAINDICATIONS • Данная вакцина индуцирует иммунитет только против менингита, вызываемого менингококками серогрупп А и С и не обеспечивает защиты от гнойных менингитов иной этиологии: менигококков группы В, Haemophilus influenzaе, Streptococcus pneumoniae и др. • Не вакцинировать детей младше 18 месяцев во внеэпидемический период.
Беременность и лактация • Изучения безвредности вакцинопрофилактики менингококковой инфекции, вызываемой менингококками серогрупп А и С для беременных женщин не проводилось. • Однако вакцинация в период беременности и лактации не является категорически противопоказанной и может проводиться в случае высокого риска инфицирования, т.е. в период эпидемии.
УСЛОВИЯ ХРАНЕНИЯ ВАКЦИН • Хранить при температуре от +2°С до +8°С (в холодильнике). • Срок хранения составляет 3 года.
Иммунитет • Иммунизация полисахаридной вакциной приводит к быстрому (с 5 по 14-й день) нарастанию антител, невосприимчивость сохраняется у детей в течение не менее 2 лет; у взрослых антитела после вакцинации сохраняются до 10 лет. Повторная вакцинация проводится не ранее, чем через 3 года. • Конъюгированные вакцины иммуногенны у детей старше 2 мес., подростков и взрослых, они создают существенно более напряженный иммунный ответ у детей и подростков. Кроме того, в отличие от не конъюгированных вакцин, они индуцируют развитие иммунологической памяти.