Download
1 / 4
40 likes | 257 Views
Psoriasis is a skin condition getting rampant in today's day and age. Read this article and have all your questions on psoriasis answered. What causes psoriasis, its types, and its treatment.

E N D
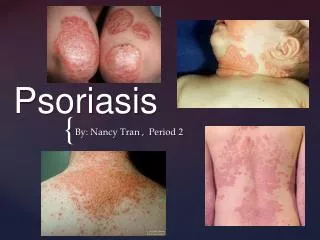
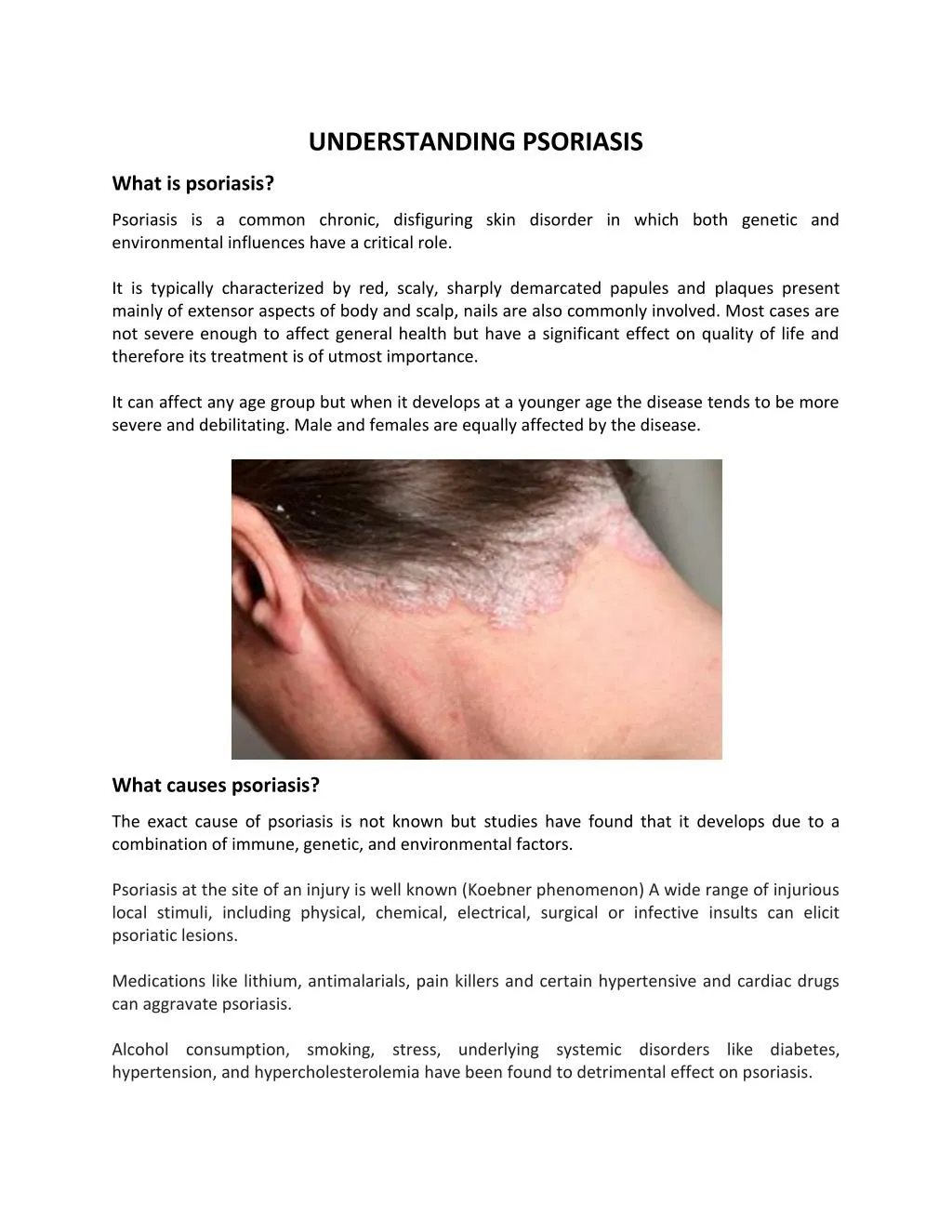
UNDERSTANDING PSORIASIS What is psoriasis? Psoriasis is a common chronic, disfiguring skin disorder in which both genetic and environmental influences have a critical role. It is typically characterized by red, scaly, sharply demarcated papules and plaques present mainly of extensor aspects of body and scalp, nails are also commonly involved. Most cases are not severe enough to affect general health but have a significant effect on quality of life and therefore its treatment is of utmost importance. It can affect any age group but when it develops at a younger age the disease tends to be more severe and debilitating. Male and females are equally affected by the disease. What causes psoriasis? The exact cause of psoriasis is not known but studies have found that it develops due to a combination of immune, genetic, and environmental factors. Psoriasis at the site of an injury is well known (Koebner phenomenon) A wide range of injurious local stimuli, including physical, chemical, electrical, surgical or infective insults can elicit psoriatic lesions. Medications like lithium, antimalarials, pain killers and certain hypertensive and cardiac drugs can aggravate psoriasis. Alcohol consumption, smoking, stress, underlying systemic disorders like diabetes, hypertension, and hypercholesterolemia have been found to detrimental effect on psoriasis.
In women hormonal factors can worsen or even improve the skin condition. What are the types of psoriasis and which parts of body are affected? The typical form is chronic plaque psoriasis where patient presents with red, well defined plaques with characteristic silvery scales which on removal leave behind pinpoint bleeding, seen predominantly on the extensor aspect of arms and legs. Other forms include pustular, erythrodermic (entire body appears red with scaling and generally patient is sick and needs hospitalization), palmoplantar (palms and soles being involved with red, scaly plaques), flexural (skin folds being affected). Scalp psoriasis is also a common form where patient has well defined plaques to diffuse scaling on scalp. Hair loss (alopecia) can occur put there is no permanent scarring alopecia and once scalp lesions resolve with treatment normal hair growth occurs. Nails can also be affected in psoriasis ranging from appearance of pits, nail discoloration, thickening and at times destruction. Psoriatic arthropathy is an entity where bones and joints get affected by the disease and patient presents with joint pain, swelling, deformity and restriction of movement. These patients may or may not have psoriatic skin lesions. Can psoriasis be completely cured? No, psoriasis is not a completely curable disease. The disease can be kept under control topical therapy, phototherapy and systemic therapies. The lesions can completely resolve with treatment over a period of time but can recur either immediately or several years after stoppage of treatment. What are the treatment options for psoriasis? For most patients, the initial decision point around therapy is between topical and systemic therapy. However, even patients on systemic therapy will likely continue to need some topical agents. Topical therapy provides symptomatic relief, minimizes required doses of systemic medications, and may even be psychologically cathartic for some patients. For purposes of treatment planning, patients may be grouped into mild-to-moderate (5-10% of the body surface area involved) and moderate-to-severe disease (more that 10% of body surface area) categories. Limited, or mild-to-moderate, skin disease can often be managed with topical agents, while patients with moderate-to-severe disease may need systemic therapy. The location of the disease and the presence of psoriatic arthritis also affect the choice of therapy. A) Mild-to-moderate disease— Limited plaque psoriasis can be treated topical corticosteroids and emollients.
Emollients are basically lotion, creams or ointments which prevent the skin from drying up. They help to keep the skin hydrated and minimize itching and irritation thus controlling development of new plaques and helping to clear out the active lesions. Alternative topical include vitamin D analogs, such as calcipotriene and calcitriol, tar, and topical retinoids (tazarotene). For facial and skin fold lesions, topical tacrolimus or pimecrolimus may be used as alternative, adjuvant or as corticosteroid sparing agents. B) Severe disease— severe psoriasis requires phototherapy or systemic therapies such as retinoids, methotrexate, cyclosporine, or biologic immune modifying agents. Phototherapy — Ultraviolet (UV) irradiation has long been recognized as beneficial for the control of psoriatic skin lesions.UV radiation acts via antiproliferative and anti-inflammatory effects thus reducing the scaling and thickness of the plaques. Both UVA and UVB light are used for phototherapy. C) Scalp psoriasis– Treatment mainly involves using a tar and salicylic acid based shampoos which help to reduce the scaling followed by use of corticosteroid in forms of lotions, foams or sprays. Phototherapy (eg, excimer laser) and systemic agents are additional treatment options for patients who cannot achieve sufficient improvement with topical agents. D) Nail psoriasis— Despite advances in the treatment of cutaneous disease, the treatment of psoriasis of the nails remains difficult. Topical and intralesional steroids, Vitamin D analogues have been used .Oral retinoids, methotrexate,cyclosporine and biological have been utilized with some success. E) Saltwater baths— As discussed above, exposure to natural sunlight has been observed to improve psoriasis. Bathing in sea water in combination with sun exposure (climatotherapy) has also been used as a therapy for psoriasis, as has the use of salt water baths with artificial UV exposure (balneophototherapy). Points to remember:- 1)Psoriatic skin needs special care to prevent dryness, irritation and thickening of skin. Use a mild soap which helps to maintain skin hydration and moisture. Avoid hot water bath as it dries the skin further. Immediately after bath apply a good emollient like petroleum jelly or thick cream to keep skin soft and supple. 2)Do not use corticosteroids for long duration in order to prevent steroid induced complications like skin thinning, striae, post inflammatory hypopigmentation. Instead
switch or combine with steroid sparing agents like Vitamin D analogue, retinoids etcetera. 3)Be careful with medications, avoid lithium based drugs .Avoid alcohol and smoking. 4)Do yearly checks of sugar, lipid levels, and monitor blood pressure. 5)Finally psoriasis per se can cause stress, low self esteem and depression and this in turn can aggravate the disease so lead a stress free and healthy live. De-stress yourself with meditation, exercise or any hobby and let the disease not overpower your mind. Source: http://www.skinclinicbangalore.com/post/understanding-psoriasis/2074