Download
1 / 35
350 likes | 388 Views
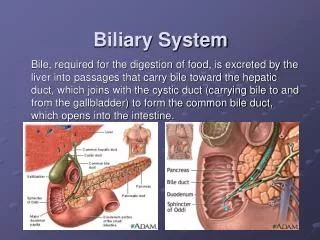
Biliary Imaging. By Dr/Ahmed Kahaar Ass. Lecturer of General surgery. Clinical Scenario. A 46 year old woman presents to the clinic complaining of epigastric pain that she experiences after eating a large meal.

E N D
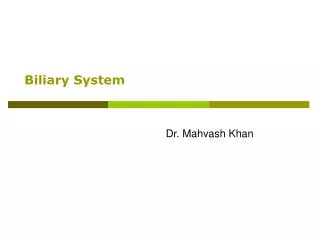
Biliary Imaging By Dr/Ahmed Kahaar Ass. Lecturer of General surgery
Clinical Scenario • A 46 year old woman presents to the clinic complaining of epigastric pain that she experiences after eating a large meal. • On examination, the patient is an obese female who does not appear to be in any acute distress. She is afebrile, with stable vital signs. The exam is only significant for the patient experiencing mild tenderness upon palpation of the right upper quadrant of her abdomen.
ACR Appropriateness Criteria • For a patient with acute right upper quadrant pain, who is afebrile with a normal WBC count:
Ultrasound Abdomen • The imaging modality of choice for the gallbladder is ultrasound. It is fast, real-time, non-invasive, and does not utilize ionizing radiation. • 95% sensitivity for detection of cholelithiasis. Diagnosis based on visualization of a mobile, hyperechoic, intraluminal mass with acoustic shadowing. • >90% sensitivity for detection of acute cholecystitis. Diagnosis based on presence of cholelithiasis, gallbladder wall thickening, pericholecystic fluid, and a sonographic Murphy sign. • Limited by skill of operator, and pt’s body habitus.
Acute cholecystitis – notice increased gallbladder wall thickness
CT scan, abdomen • Gallstones can be seen on CT, but it is not used primarily for this purpose. • CT can be used in situations where ultrasound is difficult – such as in obese patients. It can also be used if the ultrasound is not definitive.
Nuclear medicine studies • Performed using 99mTC-labelled N-substituted iminodiacetic acid compounds (99mTC-HIDA). • Can be used to detect low-grade biliary obstructions, acute cholecystitis, biliary leaks, and internal fistulas. Not used for these as often, but it is still useful for the evaluation of biliary dyskynesia or sphincter of Oddi dysfunction.
Normal hepatobiliary scintigraphy • A: liver parenchyma • B: gallbladder • C: small bowel • D: common bile duct • E: intrahepatic bile duct
Scintigraphy in acute cholecystitis. The liver is visualized, as is excretion of bile through the intrahepatic bile ducts, the common bile duct and small bowel. The gallbladder is not seen.
X-ray of the Abdomen • This was an imaging technique used in the past, but has been widely replaced by the ultrasound. • Can be used to visualize calcified stones, emphysematous cholecystitis (gas within the wall of the gallbladder), biliary fistula (gas within the biliary system), or a porcelain gallbladder.
Abdominal x-ray film, showing a “porcelain gallbladder.” This is the term used to describe a gallbladder with a calcified wall.
Oral Cholecystography (OCG) • OCG used to be the imaging modality of choice for detecting cholelithiasis. It is now used as an adjunct to ultrasound. It is obtained when the pt has the symptoms of cholelithiasis, but a negative ultrasound. • It is more useful that ultrasound for visualizing large stones, and also is useful for counting the number of stones present. • Contraindications: Pts with bilirubin > 3mg/dL, or in pregnancy.
Percutaneous Transhepatic Cholangiogram (PTC) • PTC is indicated when percutaneous intervention is needed and ERCP either is inappropriate or has failed. • Can be used to drain biliary obstructions.
PTC after injection of dye, showing a large gallstone trapped in the duct.
PTC: The same duct as before, after removal of the stone through the drainage catheter.
Endoscopic Retrograde Cholangiopancreatography (ERCP) • ERCP is the primary method of direct cholangiography, and has therapeutic potential. It also allows for examination of the upper GI tract, the papilla of Vater, and the pancreatic duct. Biopsies of multiple sites can be taken using this technique. • ERCP causes less discomfort than PTC, but acute pancreatitis is a common complication (which is rarely seen in PTC).
ERCP: The endoscope is introduced and is threaded around to the sphincter of Oddi. There, dye can be injected into the ducts. Instruments can also be inserted through the scope to remove stones, insert drains, remove tissue samples, of perform other treatments.
ERCP • The most important indication for ERCP is obstructive jaundice, as it can demonstrate the cause and extent of the obstruction. • ERCP is the preferred method of examination of patient with possible choledocholithiasis, because the stones can be extracted with balloons or gaskets after sphincterotomy is performed.
ERCP: showing slightly dilated common bile duct with calculus and normal pancreatic duct
Magnetic Resonance Cholangiopancreatography (MRCP) • MRCP is becoming a more viable imaging technique, as MRI technology improves. However, CT and ultrasound are faster, easier, and more readily available, so they are used more frequently than MRCP. • MRCP is emerging as a new tool for non-invasive evaluation of the pancreatic and biliary ductal systems. • MRCP is gradually replacing PTC and ERCP for diagnostic purposes.
References • Current Diagnosis & Treatment in Gastroenterology 2nd ed.Chapter 14: Imaging Studies in Gastrointestinal & Liver Diseases. From: StatREF • Grainger & Allison’s Diagnostic Radiology: A Textbook of Medical Imaging 4th ed.Chapter 56: The biliary tract. Churchill Livingstone: 2001. pp. 1277 – 1304. • “ACR Appropriateness Criteria for Acute Right Upper Quadrant Pain” American College of Radiology • All pictures from Google Images, www.google.com