Download
1 / 9
130 likes | 874 Views
Acute vs Chronic Subdural Hematoma. Matt Leonard MS-IV UVA School of Medicine February 2004. Clinical Data. An 88 yo WM with confusion and R facial droop found down on front steps of assisted living home HPI: h/o ground level falls PMH: HTN, CABG, GERD, Arthritis

E N D
Acute vs Chronic Subdural Hematoma Matt Leonard MS-IV UVA School of Medicine February 2004
Clinical Data • An 88 yo WM with confusion and R facial droop found down on front steps of assisted living home • HPI: h/o ground level falls • PMH: HTN, CABG, GERD, Arthritis • SH, FH, Allergies: Noncontributory • Meds: HCTZ, ASA, Terazosin, Ambien, Pepcid
Physical Exam • VS: 180/80, 79, afebrile, 94% • Neuro: Awake, alert, oriented x 3, Pupils irregular, but reactive, R facial asymmetry, bilateral symmetric motor function
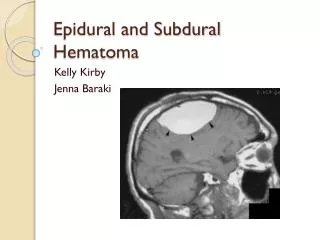
Initial CT w/out contrast SDH SDH SAH
Diagnosis • Bilateral Acute SDH’s • SAH • Frontal Contusion vs IPH
Within 24 hours Decreased LOC, Pupil inequality, motor deficit Hyperdense on CT Tx: Surgical Evacuation Greater than 2 weeks Subtle signs, weakness or hemiparesis Isodense or hypodense to brain parenchyma Tx: Symptomatic= Surgical Evacuation, Otherwise= Observation Acute vs Chronic SDH
Hospital Course • Pt. was admitted to ICU. Bilateral SDH’s were allowed to liquefy before attempted drainage. Three bore holes drilled, 2 left/1 right. Due to post-op coagulopathy, pt. was given multiple FFP doses. Pt’s coagulopathy recovered and he was discharged with neurologic deficit attributed to long inpatient stay.
References • ACR: 13.43 • References: • Marx: Rosens Emergency Medicine: Concepts and Clinical Practice. 5th edition. Mosby 2002. pp. 309-310 • Ferri: Ferri’s Clinical Advisor; Instant Diagnosis and Treatment. 2004 ed. Mosby 2004. p 813.