Download
1 / 15
150 likes | 322 Views
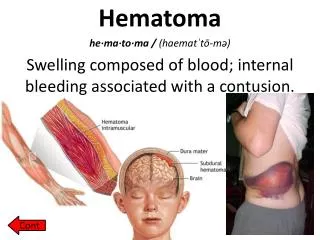
Infantil infected chronic subdural hematoma. Case presentation Helene Hurth, MS6 Innsbruck Medical University. M.M. H&P: 5 m.o . male: fever , irritability for 3 days , intermittent emesis poor hygiene , macrocephaly no h/o trauma , no LOC

E N D
Infantil infectedchronicsubduralhematoma Casepresentation Helene Hurth, MS6 Innsbruck Medical University
M.M. • H&P: 5 m.o. male: fever, irritabilityfor 3 days, intermittentemesis poorhygiene, macrocephaly no h/o trauma, no LOC alert, moves all extremities, PERRL, EOMI, bulgingfontanelle, Temp: 40,6°C (105,1°F), BP 82/67mmHg, HR 180, RR 34, SpO2 99% no ecchymosis/lacerations/abrations/deformities/crepitus • Lab: CRP 40,3 mg/dl, WBC 14,8 • PMH:termborn, methamphetaminepos at birth PICU at 1 monthfor RSV, apneaspells • SH: fatherretainsfullcustody open CWS case – mother: substanceabuse 3y/o healthysibling
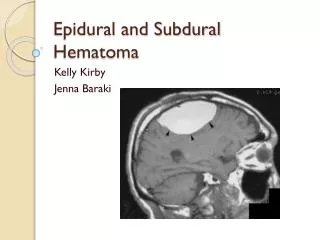
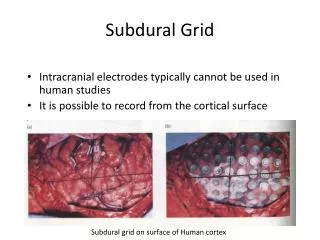
Preoperative MRI Bilateral chronic subduralhematoma Le: 25 mm Ri: 15 mm Enhancement of membranes 3mm rightward midlineshift
M.M. • Subduraltab via AF afteradmission: 4+ GNR in gram stain – E.coli • Burr hole drainagew/ bilateral drainsthenextmorning • Abx: Ceftriaxone, Meropenem
Postoperative MRI Le: 12 mm Ri: 7-8 mm Resolution of midlineshift Septations
OP • Craniotomy w/ resection of membraneson day 5 afterborr hole drainagedue to remainingfever and up trendinginflammatorymarkers
Childhood extraaxial CNS infections • Age peaks: >11y (50%) & <1y (>20%) • Duration of symptoms based on underlying cause • Fever, headache, altered consciousness, focaldeficits, full AF, poorfeeding, seizures S. Gupta, J NeurosurgPediatrics 2011
Childhood extraaxial CNS infections • Postsinusitis: (frontal) SDE, epiduralabscess, Pott‘spuffytumor; +- cerebritis • Postmeningitis: diffuse hemispheric/infratentorial SDE • Postoperative: epidural abscess, SDE, osteomyelitis at OP-site • Otogenic-> mastoiditis: SDE, epiduralabscess S. Gupta, J NeurosurgPediatrics 2011
Childhood extraaxial CNS infections • Treatment: Initial widecraniotomy + abx • Complications: recurrentseizures, venoussinus/ corticalveinthrombosis • Outcome: preoperativepresentation Etiology early, aggressive surgicaltreatment S. Gupta, J NeurosurgPediatrics 2011
Infected CSDH • Rare • Streptspp, Staphaureus, H. influenzae, E. coli, Salmonellaspp • Hematogenous • Satisfactoryoutcome • Antibiotictreatment • Drainage vscraniotomy
Surgicaltreatment: CSDH • Pre-OP T2*-MRI, randomly BH or SC • Burr holes: equivalent, lowermortality/morbidity/hospitalstay • Small craniotomy w/ resection of outer and intrahematomalmembranes: superiorifintrahematomalmembranespresent M. Tanikawa, Acta Neurochirurgica 2001 N=20 N=29
Surgicaltreatment: CSDH • Outcome, reoperation, hospitalstay • Hematomarecurrance: thickmembranes -> residualhematoma -> rebleeding MRI (T2*) imaging to predictneedfor craniotomy M. Tanikawa, Acta Neurochirurgica 2001
Summary • Neurosurgeryoftenrequired in extraaxial CNS infections • Earlydiagnosis! • Considerinfected CSDH withsigns of bacteremia