Download
1 / 42
1.02k likes | 6.54k Views
Clinical Case Study: Acute Pancreatitis. By Nicole Vantress --- February 2013. Background. Medical Presentation. Patient C.P. transferred from Grossmont Hospital for gallstone pancreatitis Admitted to UCSD CCU January 13, 2013 with respiratory distress and sepsis

E N D
Clinical Case Study: Acute Pancreatitis By Nicole Vantress --- February 2013
Medical Presentation • Patient C.P. transferred from Grossmont Hospital for gallstone pancreatitis • Admitted to UCSD CCU January 13, 2013 with respiratory distress and sepsis • Length of stay: 1/13/2013- present
Anthropometrics • C.P. 55 year old male • 6 ft. (72”) • 365# (166 kg) • BMI: 49.6 • Ideal Body Weight (IBW): 178# (81kg) • Percent IBW (%IBW): 205% • PMH: HLD, HTN, nephrolithiasis, BPH (benign prostatic hyperplasia), and morbid obesity
Prior to Admission • Symptoms • Back pain upper abdominal pain • Pain worsened with food • Nausea and emesis • Fevers and chills • Decreased urine output • Social History/ Other History • Gallstones • 2 glasses of wine twice a week • No past history of pancreatitis • Lives with partner and daughter • Good job, no stressors
Medical Status at Admit to CCU • Gallstone pancreatitis with severe sepsis • AKI • Transaminitis • Plural effusion • Atelactasis vs developing PNA • Hyperglycemia • Hemodynamically unstable • NPO
Progress from Admit to Initial Nutrition Assessment • Pt intubated 1/14 • Sedated and started on 3 vasopressors (norepinephrine, phenylephrine, vasopresson) • Started CRRT 1/14 • Coretrack
Coretrack • Imaging note: “Coretrack placed with tip in atrum.” • Not appropriate with pancreatitis
Vasopressors • Patient on norepinephrine, phenylephrine and vasopressin. • Vasoconstriction and decreased oxygenation to the gut and microvili put the patient at higher risk for nonocclusive bowel ischemia. • 3 pressors hold • 2 pressors trophic feeds • 1 pressor advance TF slowly
Obesity in the ICU • Hypocaloric feeding when BMI >30 • 60-70% of target energy • If over age 65, Penn State Equation already factors this percentage in. • High protein needs • For ventilated, critically ill patients: • BMI<30: 1.2-2.0 gm/kg actual weight • BMI 30-40: 2.0 gm/kg IBW • BMI > 40: Greater than or equal to 2.5 gm/kg IBW • ~2 g/kg might not be indicated in liver and renal impairment • Patient on CRRT so not a concern.
Sepsis • Hypocaloric feeding the first week of sepsis • 55-65% of goal kcal • Then feed REE x 1.5 for calories • 1.5-2 g/kg protein • Increased needs can reamain elevated for up to 21 days even when sepsis has been treated.
CRRT (Continuous Renal Replacement Therapy) • CRRT removes water and wastes at a slow and steady rate (usually over 24 hrs). • Who gets CRRT?
CRRT cont. • Goals of CRRT • To correct electrolyte and metabolic imbalances associated with renal dysfunction • Maintain optimal fluid balance • Types/dialysate • SCUF (Slow Continuous Ultrafiltration) • CVVHDF (Continuous Venous-Venous HemoDiaFiltration) • CVVH (Continuous Venous-Venous Hemofiltraition) • CVVHD (Continuous Venous-Venous Hemodialysis • % glucose in dialysate ranges from 0.1%-2.5%. • UCSD uses 0.1%, which only provides 33 kcals.
CRRT Cont. • Nutrition goals • Oral and enteral diet does not usually need to be restricted for renal • Protein needs usually range from 1.5-2.5 g/g (more accurate estimate can be calculated from 24 hour data) • Renal MVI for water-soluble losses • Standard formula is appropriate • Insulin drip
CRRT Calculation for Protein Needs • In lab values, under filtrate tabs, find BUN ultrafiltrate. Start with lab value from day before and two others previous from that. Add up and take avg. • Only able to do calculation if all three values are within 10 points of each other. • Under CRRT flowsheet: • Make sure the is a number for each hour of the day yesterday 0000-2300. • Add up all the numbers from dialysate infused (1B) • Add up all the numbers in the patient fluid removal (3A)
CRRT Calculation Cont… • Take (1B) + (3A) = TOTAL • TOTAL x BUN Avg = XYZ • Take (XYZ/100/1000) + 4 + 1.5 (g of nitrogen lost per 24 hrs) = g nitrogen • G nitrogen x 6.25 (6.25g nitrogen in 1g protein) = g protein • Can add g nitrogen + 2, then multiply by 6.25 to make a protein range
Significant Labs at Initial Assessment • No prealbumin or CRP • Elevated LFTs • K+/P/Mg WNL
Nutrition RequirementsEstimated Needs • Energy • REE per Penn State Equation: 3281 x 0.55-0.65 for sepsis/obesity = 1804-2133 kcal (22-26 kcal/81 kg IBW) • Protein • 162-203 gm protein (2-2.5 g/81 kg IBW) • 24 hr CRRT info not available • Maintenance Fluids • 500-1000 mL + UOP or per MD given CRRT
Nutrition Care Process • Diagnosis: PT with inadequate nutrient intake R/T NPO status, hemodynamic instability/sepsis AEB diet Rx and no nutrient intake since admission. • Intervention Goal: Pt to receive > 75% of estimated nutrient needs with acceptable tolerance.
Nutrition Plan/ Recommendations • Start senna/colace. • LBM prior to admission • D/C coretrack and place NJ tube via IR if/when possible. • pancreatitis • REC once on 2 pressors or less, start Peptamen AF @ 10 mL/hr x 24 hrs. • why the low goal rate? • Continue calcium gluconate. • Note low ionized Ca • REC check prealbumin along with CRP to get baseline, then weekly to trend and to better assess nutrition status. • Check weight daily to monitor trends/dry weight.
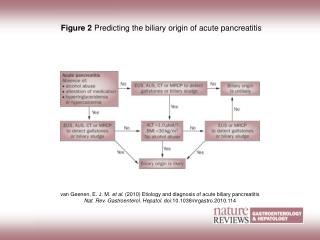
Gallstone Pancreatitis • Gallstone pancreatitis is inflammation of the pancreas that results from blockage of the pancreatic duct by a gallstone. • 15% of cases of acute pancreatitis are either idiopathic or from biliary disease. • Progression of disease • Obstruction blocks enzymes • Pancreatic enzymes • Amylase and lipase
LFTs • Obstructed outflow • Elevated alkaline phosphatase, ALT, AST, and bilirubin • ALT >150 IU/L • C.P. had these elevated liver enzymes • Progress note: • MD noted LFTs had begun to trend down, which suggests the gallstone had passed.
Risk Factors • Female gender • Obesity • Older age • High cholesterol levels • Rapid weight loss • Diabetes • Pregnancy
Severe acute pancreatitis • The mean hospital length of stay is approximately 1 month • Organ failure occurs in at least 16% to 33% of cases, and infection complicates the disease course in 30% to 50%. • Mortality alone is 19% to 30%, but may range up to as high as 80% if organ failure or sepsis complicates the disease process.
Treatment • Pancreatic Rest • Severe pancreatitis • Nutrition support • Fix underlying cause
PN vs EN • Need for pancreatic rest can still be achieved with EN • EN reduces: • infectious morbidity • hospital length of stay • cost for nutrition support • need for surgical intervention • multiple organ failure and mortality • Feeding the gut
Early Enteral Feeds • Feeding within 24-48 hours showed the most outcome benefits • EN should be initiated as soon fluid resuscitation is complete • Less gut permeability • Decreased release of inflammatory cytokines • Overall decrease in infectious morbidity and hospital length of stay
Tube Feed Placement and Formula • NJ preferred with severe acute pancreatitis • 40 cm or more below the Ligament of Treitz • Coretrackvs IR placement • Peptide based formula • Peptamen AF • Other options • Nepro • Standard formula (2 cal)
Nutrition Goals • Increased energy expenditure and protein catabolism • Calories: 22-47 kcal/kg or injury factor of 1.3-1.5 x REEProtein: 1.4-2 g/kg protein • End goal of low fat PO diet
Patient progress • Gallstone passed • Staged wounds • Stage 2 • REC nephrocaps • Feeding at goal rate • Peptamen @ 65 mL/hr + Prosource TID • Lipase back to normal
Complications • (1/26) Decreased goal rate to Peptamen @ 40 mL/hr • Diarrhea per MD; improved when tube feeds were held • Placement of FT still not optimal • (1/24) Imaging showed tip in duodenum, (1/25) imaging showed poorly visualized tip of the feeding tube • Left in duodenum because lipase, LFTs decreased • REC NJ for best tolerance • Couldn’t wean off ventilator, vasopressors or CRRT • Sepsis, necrotizing pancreatitis or both.
Patient Progress Cont. • Moved to SICU and put on surgical team service • Necrotizing pancreatitis • REC pancreatic enzymes-creon for better absorption • REC goal rate @ 65 mL/hr + Prosource TID • Necrosectomy (1/30) and repeat necrosectomy (1/31) • (2/4) Abdominal washout, debridement of necrotic pancreas, cholecystectomy, and temporary abdominal closure.
Monitoring/Evaluation • Labs • Prealbumin/CRP
Monitoring/Evaluation Cont • Labs • Lipase/amylase • Renal labs now switched to iHD • Wounds • Remains staged 2; improving • Wt/fluids • D/C CRRT, trending up
End Nutrition Goals • NJ feeding of Peptamen @ 65 mL/hr x 24 hrs + prosource TID • ADAT to PO low fat diet • Possible need for pancreatic enzymes, regular diet
References 1. The A.S.P.E.N. nutrition support core curriculum: A case-based approach-The adult patient. ASPEN. 2007. 2. Inotropes and vasopressors. Contemporary review in cardiovascular medicine. Circulation 2008. 3. Wells DL. Provision of enteral nutrition during casopressor therapy for hemodynamic instability: An evidence-based review. Nutrition in Clinical Practice. 2012; 27:521-526. 4. Choi Y, Silverman WB. Biliary tract disorders, gallbladder disorders, and gallstone pancreatitis. American College of Gastroenterology. 2013. 5. Norman JG. New approaches to acute pancreatitis: role of inflammatory mediators. Digestion. 1999;60(suppl 1): 57-60.
References Cont 6. Ed. Gottschlich, MM. The A.S.P.E.N nutrition support core curriculum: A case-based approach-The adult patient. ASPEN. 2007. 7. Petrov MS, Kukosh MV, Emelyanov NV. A randomized controlled trial of enteral versus parenteral feeding in patients with predicted severe acute pancreatitis shows a significant reduction in mortality and in infected pancreatic complications with total enteral nutrition. Dig Surg. 2006;23:336-344. 8. Eckerwall GE, Axelsson JB, Andersson RG. Early nasogastric feeding in predicted severe acute pancreatitis: a clinical, randomized study. Ann Surg. 2006;244:959-967. 9. Casas M, Mora J, Fort E, et al. Total enteral nutrition vs. total parenteral nutrition in patients with severe acute pancreatitis. Rev EspEnferm Dig. 2007;99:264-269.