Download
1 / 33
330 likes | 349 Views
Tendinopathies in the Hand. Goal. To review common tendinopathies in the hand Terminology Pathology S pecific conditions and treatments. Terminology and Pathology. Tendinopathy. Painful conditions affecting the tendons of the wrist hand Most common reason for hand surgeon visit

E N D
Goal • To review common tendinopathies in the hand • Terminology • Pathology • Specific conditions and treatments
Tendinopathy • Painful conditions affecting the tendons of the wrist hand • Most common reason for hand surgeon visit • Entrapment/stenosis vs. Inflammation • Trigger finger De Quervains vs. • Rheumatoid associated tenosynovitis
“Tendinosis” • Histology: • collagen degradations, • absence of inflammatory cells • vascular ingrowth • Accumulation of micro-ruptures • Associated pain • possibly from neurochemical cytokines (substance P, glutamate, others) • potentiated by vascular ingrowth
“Tendon entrapment/Tendovaginitis/Stenosing tendovaginitis” • Entrapment • Thickening of tendon sheath • Fibrocartilagenous metaplasia • Tendinosis
“Tenosynovitis” • Inflammation of synovial lining of tendon sheath • Typically assocat4d with inflammatory arthropahies(RA) • Deposition diseases • Amyloid, calcific tendonitis/gout, septic
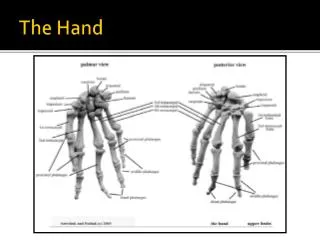
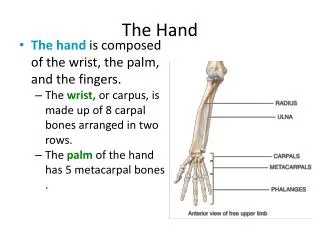
Tendon anatomy • Enter a fibro-osseous tunnel (flexor sheath) at the level of the MCP joint • Sheath thickened to produce strong annular pulleys that position the tendons close to the underlying bone • A2 and A4 pulleys are essential to prevent bowstringing
Flexor Tendons Annular and Cruciate Pulleys Essentials of Hand Surgery 2002
Extensor tendons • Compartments • 1st- APL & EPB • 2nd- ECRL & ECRB • 3rd- EPL • 4th- EIP & EDC • 5th- EDQ • 6th- ECU Essentials of Hand Surgery 2002
Trigger finger“Stenosing tendovaginitis” • Often called “stenosing tenosynovitis: • A1 pulley entrapment by enlarged tendons • Fibrous metaplasia of A1 pulley • Tendinosis like changes in tendon
Trigger finger“Stenosing tendovaginitis” • Women 6:1 • 3% lifetime risk • 10-20% diabetics • Higher risks hypothyroid, renal dz, rheumatological, gout • Pain, clicking, catching, limited grip • Concordant with CTS
Trigger finger“Stenosing tendovaginitis” • Treatment • NSAIDs • Splinting/Therapy • Injections • Surgery
Trigger finger“Stenosing tendovaginitis” • Splinting/Therapy • Some have shown it works • 44% improvement • 55% resolution DIP splinting • If respond to therapy have less recurrence at 6mo
Trigger finger“Stenosing tendovaginitis” • Injection • Location of injection/technique • No difference in effectiveness • Possible worse side effects if subq • Atrophy, pulley rupture, tendon ruputre • Cure in 57-97% (1-2 injections) ~ 80% cure • Less success with more injections • Recurrence higher with multiple digits, younger, diabetes
Trigger finger“Stenosing tendovaginitis” • Injection • Diabetic • 57-86% cure • Less effective if poor glucose • Elevate serum glucose • Type of steroid • Insoluble (triamcinolone) *more rapid • Soluble (dexamethasone) *more durable
Trigger finger“Stenosing tenosynovitis” • Splinting/Therapy • Some have shown it works • 44% improvement • 55% resolution DIP splinting • If respond to therapy have less recurrence at 6mo
Trigger finger“Stenosing tendovaginitis” • Surgery • Percutaneous release • ? Equal efficacy • Injury to neurovascular bundle, A2 pulley, incomplete release • Usually ok middle ring
Trigger finger“Stenosing tendovaginitis” • Surgery • Open release • A1 pulley release • *Not in rheumatoid arthritis • Low threshold for FDS tenectom
“Extensor tenovaginitis” • Dequervains • Intersection syndrome • ECU tenosynovitis
Extensor tendon anatomy • Compartments • 1st- APL & EPB • 2nd- ECRL & ECRB • 3rd- EPL • 4th- EIP & EDC • 5th- EDQ • 6th- ECU Essentials of Hand Surgery 2002
“Dequervains” • Dequervains • Impaired gliding of APL EPB • Myxoid degeneration, muco-polysaccharide deposition, fibrocartilage metaplasia • 1.3% women, 0.% men
“Dequervains” • Dequervain’s • Associated • Pregnancy • Postpartum • Lactation • Finklestein • Ulnar deviation • Treatment • NSAIDs • Splinting (14%) • Injection (60%) • Surgery
“Dequervains” • Dequervains • Steroid atrophy • Superficial radial sensory nerve branch • Subluxaition of tendons
“Intersection syndrome” • Intersection syndrome • Where 1st and 2nd cross (more proximal) • Rowers and gymnasts
“EPL/EDC tenosynovitis” • Rare
“ECU tenosynovitis” • Usually twisting injury • Concomitant injury with TFCC injury • ECU subluxation • Dynamic ultrasound • Treatment • RICE • Therapy • Occasional operations For tenoysynovectomy or subluxation
“ECU tenosynovitis” • Usually twisting injury • Concomitant injury with TFCC injury • ECU subluxation • Dynamic ultrasound • Treatment • RICE • Therapy • Occasional operations For tenoysynovectomy or subluxation
“FCU/FCR tenosynovitis” • These are repetitive injury • Can be calcific • FCR with STT arthritis • NSAIDS, RICE, steroids • ?rupture/ rare surgical • release