Download
1 / 30
390 likes | 898 Views
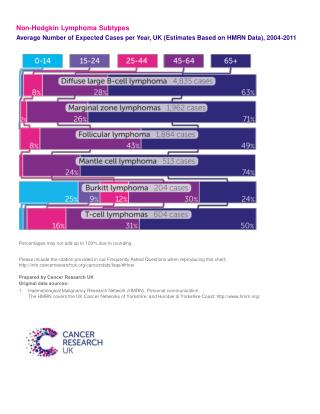
Update on T-cell Non-Hodgkin Lymphoma in China. Huaqing Wang, M.D. Cancer Hospital and Institute of Tianjin Medical University. International Variation http://www-dep.iarc.fr/. Females. Males. 发病率 (Incidence). 亚洲国家的发病率较西方国家高,在非霍奇金淋巴瘤中的比例 15-20% 一项国际性回顾研究评估了北美、欧洲和亚洲 22 个地区

E N D
Update on T-cell Non-Hodgkin Lymphoma in China Huaqing Wang, M.D. Cancer Hospital and Institute of Tianjin Medical University
International Variationhttp://www-dep.iarc.fr/ Females Males
发病率 (Incidence) • 亚洲国家的发病率较西方国家高,在非霍奇金淋巴瘤中的比例 15-20% • 一项国际性回顾研究评估了北美、欧洲和亚洲22个地区 1314例T细胞淋巴瘤* *Arimitage.International Peripheral T-Cell and Natural Killer/T-Cell Lymphoma Study: Pathology Findings and Clinical Outcomes. J Clin Onco2008; 26(25):4124-30
Trends in incidence of PTCL by subtype from 1992 to 2005, 13 SEER registries PTCL incidence increased by 280%. Abouyabis et al., Leuk & Lymphoma 2008;49:2099
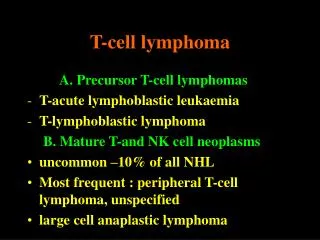
T-cell Lymphoma Classification: WHO Predominantly leukemic/disseminated T-cell prolymphocytic leukemia T-cell large granular lymphocytic NK/T-cell leukemia/lymphoma Adult T-cell leukemia/lymphoma Predominantly nodal Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma Peripheral T-cell lymphoma (Unspecified) Predominantly Extranodal Mycosis Fungoides Sezary syndrome Primary cutaneous CD30+ disorders Anaplastic large cell lymphoma Lymphomatoid papulosis Subcutaneous panniculitis-like T-cell NK/T-cell lymphoma-nasal Enteropathy-type intestinal lymphoma Hepatosplenic T-cell lymphoma Precursor T/NK Neoplasms Precursor T lymphoblastic leukemia/lymphoma Blastic NK lymphoma Peripheral T/NK Neoplasms
天津地区20年恶性淋巴瘤的发病率 天津医科大学肿瘤医院回顾性了分析1986~2005年天津地区20年恶性淋巴瘤的发病情况: 外周T细胞占非霍奇金淋巴瘤的比例高达34%, 外周T细胞非特指型为10.8%, NK/T细胞淋巴瘤为14.9%, 皮肤T细胞淋巴瘤为2.0%, 肠病型T细胞淋巴瘤为0.5%。
Known Risk Factors • Immune modulation • Congenital immunodeficiencies • Immunosuppression • HIV • Autoimmune disorders • Infectious organisms • Human T-cell lymphotrophic virus • (HTLV-1) - ATLL • Epstein-Barr virus (NK/T-cell, AITL?) • H Pylori • Familial aggregation
…. the Remaining Cases of NHL • Environmental factors (e.g., pesticides, solvents, PCBs) • Lifestyle factors • Obesity • Diet • Alcohol • UV light • Genetic factors
St. Bartholomew’s Hospital, London Guy's and St Thomas, London Newcastle University Christie Hospital, Manchester Southampton University Royal Wolverhampton Hospitals NHS Trust Nebraska University Cleveland Clinic Memorial Sloan Kettering CC Stanford University NCI MD Anderson Yale-New Haven CC Utah University Nashville-Vanderbilt UMC CALGB Columbus-Ohio National Oncological Institution (NOU) GELCAB Czech Lymphoma Study Group SAKK Moscow-Cancer Research Center of RAMN IIL GOL GITIL GISL/NHLCSG GIMURELL GR. TOSCANO GR. RO/BO HOST IEO Programa Nacional de Cancer del Adulto Chile (PANDA) Santiago de Chile – Hospital del Salvador Queen Mary Hospital (GATLA) Grupo Argentino de Tratamiento de la Leucemia Aguda Buenos Aires – FUNDALEU La Plata – Hospital San Martin GEMOH Brazil University of Campinas Sao Paulo-Santa Casa Medical School Tel Hashmer Sheba Medical Center Tel Aviv Sourasky Medical Center Beilinson Medical Center Rambam Medical Center Shaare Zedek Medical Center Uruguayan Society of Hematology (SHU) Montevideo-Hospital Maciel Samsung Medical Center Seoul
International T-cell NHL Study: Sites (N = 1314) • North America • Vancouver, Bethesda (NCI), Nebraska, Massachusetts (MGH), California (USC), Arizona • Europe • Barcelona, Norway, Wuerzburg, London, Lyon, Leeds, Madrid, Bologna, Modena • Asia • Bangkok, Hong Kong, Singapore, Tokyo, Nagoya, Okayama, Fukuoka, Seoul
Overall and Failure-free Survival PTCL-NOS Cases 1.0 0.9 0.8 0.7 0.6 Proportion 0.5 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Time CENSOR FAIL TOTAL MEDIAN FFS 72 261 333 0.91 OAS 112 221 333 2.01
Overall Survival PTCL-NOS Cases by IPI Test: p<0.001 1.0 0.9 0.8 0.7 0.6 Proportion 0.5 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Time IPI CENSOR FAIL TOTAL MEDIAN 0/1 36 47 83 5.03 2 36 67 103 2.1 3 20 53 73 1.41 4/5 9 38 47 0.68
Overall Survival PTCL-NOS Cases by Anthracycline Initial Tx 1.0 0.9 Test: p=0.14 0.8 0.7 0.6 0.5 Proportion 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Time Anthracycline as part of initial tx CENSOR FAIL TOTAL MEDIAN yes 98 173 271 2.1 no 14 34 48 1.57
Failure-free Survival PTCL-NOS Cases by Transplant Reason 1.0 0.9 Test: p<0.001 0.8 0.7 0.6 0.5 Proportion 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 Time Transplant reason CENSOR FAIL TOTAL MEDIAN inital tx 8 15 23 1.46 subseq. to recur. 0 24 24 0.71
Overall and Failure-free Survival Anaplastic large cell lymphoma, ALK+ 1.0 0.9 0.8 0.7 0.6 Proportion 0.5 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Time Survival CENSOR FAIL TOTAL MEDIAN FFS 45 32 77 10.4 OAS 56 21 77 .
Overall and Failure-free Survival Anaplastic large cell lymphoma, ALK- 1.0 0.9 0.8 0.7 0.6 Proportion 0.5 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Time Survival CENSOR FAIL TOTAL MEDIAN FFS 30 39 69 1.33 OAS 36 33 69 4.49
Overall and Failure-free Survival NK/T-cell lymphoma, nasal type 1.0 0.9 0.8 0.7 0.6 Proportion 0.5 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 Time Survival CENSOR FAIL TOTAL MEDIAN FFS 4 30 34 0.29 OAS 5 29 34 0.36
Phase II study of Bevacizumab and CHOP (A-CHOP) for patients with PTCL or NK Cell NeoplasmsECOG 2404
PROPEL: A Multi-center Phase 2 Open-label Study of Pralatrexate with Vitamin B12 and Folic Acid Supplementation in Patients with Relapsed or Refractory Peripheral T-cell Lymphoma (PTCL) O.A. O’Connor, B. Pro, L. Pinter-Brown, L. Popplewell, N. Bartlett, A. Shustov, M.J. Lechowicz, K. Savage, B. Coiffier, E. Jacobsen, P.L. Zinzani, A. Goy, J. Zain, S. Wilroy, M. Patterson, A. Boyd, M. Saunders, P. Cagnoni, S. Horwitz Blood 112: 261a, 2008
PROPEL Study IWC: International Workshop Criteria
PROPEL Histology *Two treated patients excluded from efficacy analysis
PROPELSummary of Response by Central Review: IWC 69% of responders did so after Cycle 1 C1: Cycle 1
ASH 12/2008, Abstract# 263 Clinically Significant Responses Achieved with Romidepsin in Treatment-Refractory Cutaneous T-Cell Lymphoma: Final Results from a Phase 2B, International, Multicenter, Registration Study
Romidepsin Romidepsin H O CH3 HN CH3 S HN H3C S O H O NH O HN H O CH3 CH3 O H Molecular Weight 540.71 • Novel bicyclic peptide • Potent pan-histone deacetylase (HDAC) inhibitor • Greatest activity against: • Class I (HDACs 1, 2, 8) • Class II (HDACs 4, 5, 6) • Class IV (HDAC 11) • In vitro efficacy • HUT-78 (TCL cell line) IC50 = 1.4 x 10-9M
HDAC Inhibitors: Multifunctional Anticancer Agents Acetylation of Histone and Non-Histone Proteins Altered Gene Expression And Protein Function • Apoptosis • Hsp90, Bcl-2, Bcl-XL, Bax, • Fas, Caspase-3 & 9 Angiogenesis VEGF, VEGFR, MMPs, Activin A, Ang2, eNOS • Cell Cycle Arrest • p21, p27, Cyclin A & D • Cellular Differentiation • MDR-1, Na-I Symporter, CD25, • CAR (Adenovirus Receptor), • RARα & β • Cellular Transformation • C-myc, Ras, Raf, Bcl-6, p53
Patient CharacteristicsAs-Treated Population (N=96) 71% with advanced stage (≥IIB)
Response by CTCL Clinical StageEvaluable Population (N=72) • Responses in advanced disease (stages IIB-IVA) • 48% ORR for ≥ IIB • 8 patients with Sézary syndrome, 4 (50%) had a PR
Conclusions • Single agent romidepsin is active in CTCL with an overall response rate (ORR) of 42% in evaluable patients including 6 CRs • In advanced stage disease (IIB-IVA) the ORR is 48% • ORR in stage IIB 56%, SS 50% • Pruritus relief in 63% of patients with mod-severe pruritus at baseline despite the exclusion of the use of steroids and antihistamines • Most AEs associated with romidepsin were mild (grades 1-2) and manageable • Romidepsin does not have a significant effect on the QT Interval
HDAC inhibitors Vorinostat Romidepsin LBH 589 Folate antagonists Pralatrexate Lenalidamide Syk inhibitor – R788 Proteosome inhibitors Purine analogues Gemcitabine Platinum agents Bevacizimab Campath Ontak Endostar Tranditional Chinese herbs Agents In Development for T-Cell NHL