Download
1 / 21
210 likes | 423 Views
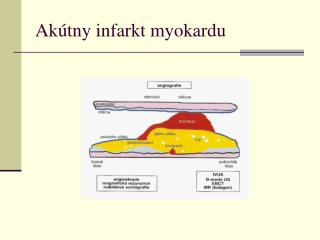
ACS/akuter Infarkt. Konkretes Vorgehen bis zur Herzkatheteruntersuchung. Definition/Klinik ACS. Instabile Angina Pectoris Ruhe-Angina mit mehr als 20 min. Dauer Neu aufgetretene Angina welche die körperliche Leistungs fähigkeit einschränkt Zunehmende Angina Pectoris NSTEMI STEMI.

E N D
ACS/akuter Infarkt Konkretes Vorgehen bis zur Herzkatheteruntersuchung
Definition/Klinik ACS • Instabile Angina Pectoris • Ruhe-Angina mit mehr als 20 min. Dauer • Neu aufgetretene Angina welche die körperliche Leistungs • fähigkeit einschränkt • Zunehmende Angina Pectoris • NSTEMI • STEMI
Kontinuum des ACS - Spontanverlauf und Definition - stabile KHK instabile Angina pectoris Myokardinfarkt KHK ACS Jahre Monate Tage Stunden
Diagnostik • Anamnese • EKG • Biochemische Parameter • Andere...
Anamnese und klinischer Befund • Leitsymptom akuter Thoraxschmerz • Ruhe-AP > 20min. Dauer prognostisch bedeutsam • Nitro (+) ? • Atypische AP bei <40 und >75Jahre, Diabetiker und Frauen • RF und frühere koronare Ereignisse • Klinische Untersuchung wenig spezifisch, gibt Anhalt für nichtkardiale Ursache
EKG • 12-Kanal EKG innerhalb von 10min. • Vergleich mit „Vor-EKG“ • ST-Senkung in mehr als zwei Ableitung mit hohem prognostischen Stellenwert • LSB und SM nur eingeschränkte Verwertbarkeit • „Normales EKG“ kein Ausschluß für ACS Quantitative T-wave analysis predicts 1 year prognosis and benefit from early invasive treatment in the FRISC II study population. Jacobsen MD, Wagner GS, Holmvang L, Kontny F, Wallentin L, Husted S, Swahn E, Stahle E, Steffensen R, Clemmensen P. Eur Heart J. 2005 Jan;26(2):103-4.
Biochemische Marker • Troponin; CK, CK/MB • „falsch positives Troponin“: • Crea >2,5 mg/dl, Myokarditis, Lungenembolie, dekompensierte Herzinsuffizienz, Hypertensive Krise, Contusio cordis, Trasplantatatabstoßung • Kombination aus NT-Pro-BNP und Crea-Clearance als bester prognostischer Marker für 1-Jahresletalität. James SK et. Al. N-terminal pro-brain natriuretic peptide and other risk markers for the separate prediction of mortality and subsequent myocardial infarction in patients with unstable coronary artery disease: a Global Utilization of Strategies To Open occluded arteries (GUSTO)-IV substudy Circulation. 2003 Jul 22;108(3):275-81.
Akuttherapie im Krankenhaus • Ziel: • Erreichen von Beschwerdefreiheit • Verhinderung von Komplikationen • Voraussetzung: • Richtige Diagnose und Risikostratefizierung
Risikopatienten • Troponin T oder I positiv • ST-Senkung (>0,1mV) • Hämodynamische Instabilität • Rhythmusinstabilität • Diabetes mellitus
TIMI risk score • Alter > 65 Jahre • Bekannte KHK, oder mindestens drei Risikofaktoren • Bekannte 50%ige Koronarstenose • ST-Strecken Veränderung im Aufnahme-EKG • Zwei oder mehr Episoden von AP während der letzten 24h • Erhöhtes Troponin oder CK/CK-MB • Einnahme von ASS während der letzten sieben Tage The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. Antman EM; Cohen M; Bernink PJ; McCabe CH; Horacek T; Papuchis G; Mautner B; Corbalan R; Radley D; Braunwald E JAMA 2000 Aug 16;284(7):835-42.
Therapieziele • Erhalt der linskventrikulären Funktion • „time is myocard!“ • Verhinderung eines weiteren Thrombuswachstums • Komplette und stabile Wiedereröffnung des Koronargefäßes
IAP/NSTEMI STEMI NSTEMI
PCI vs. Fibrinolyse (STEMI) ACC/AHA Guidelines for the management of patients with ST-Elevation myocardial infarction, 2004
PCI-Arten bei STEMI Zeitintervall Strategie Studien PCI Lyse / PCI < 3 h > PCI / Transfer LIMI, PRAGUE-1,-2, DANAMI-2, Air-PAMI, C-PORT primary < 12 h SIAM-III, CAPITAL-AMI, PRAGUE-1, SPEED, PACT, BRAVE (ASSENT-4, FINESSE) ADMIRAL, TIGER-PA, BRIDGING Lyse GP IIb/IIIa facilitated < 12 h > 60 min n. Lyse “Lyse- Versager“ RESCUE I, II, REACT rescue Schock immer SHOCK, SMASH
Therapie des ACS (IAP/NSTEMI) • O2 über Nasensonde/Maske (4–8 l/ min) • Glyceroltrinitrat 0,4–0,8 mg s. l., evtl. wiederholt u. U. Infusion 1–6 mg/h bei schwerer Linksherzinsuffizienz/(Cave RR <90 mmHg und/oder höhergradiger AV Block) • Morphin 3–5 mg i. v., ggf. wiederholt bis Schmerzfreiheit • Bei vagaler Reaktion Atropin 0,5 mg i. v., ggf. wiederholt • Bei Übelkeit/Erbrechen Antiemetika (z. B. Metoclopramid i.v.) • langwirksamer ß-Blocker (z. B. Metoprolol 5 mg langsam i. v.) Ca-Antagonisten bei KI für ß-Blocker (Verapamil oder Diltiazem) • ASS (500mg i. v.) • Heparin 70 U/kg i. v., max. 5000 U, oder: Enoxaparin 30 mg i. v.+1 mg/kg s. c.
Begleittherapie PCI • ASS • Clopidogrel/Ticlopidin • Heparin • Glykoprotein IIb/IIIa Antagonisten
Antithrombotische Begleittherapie ASS und Clopidogrel immer als Kombination! Clopidogrel additiv für 3-4 Wochen nach einfacher Stentimplantation. Clopidogrel additiv für 6-12 Monate nach DES. Beachtung der Kontraindikationen; Cave bei CABG! Guidelines for percutaneous Coronary Interventions, Eur Heart J 26: 804-847
Heparine • Schlechte Steuerbarkeit des unfraktionierten Heparins (UFH) variable Proteinbindung und Inaktivierung, häufige Kontrollen der aPTT oder ACT nötig • Niedermolekulare Heparine (LMWH) haben trotz s.c. Applikation konstantere Wirkung • keine Laborkontrollen nötig • Enoxaparin vermutlich beste Substanz und besser als UFH (30mg iv-Bolus, dann 2xtgl 1mg/kg sc. für 8 Tage) • Bei frühzeitiger Koronarintervention: • Keine Überlegenheit von NM-Heparinen
Empfehlungen für GP IIb/IIIa Antagonisten als Begleittherapie bei PCI Guidelines for percutaneous Coronary Interventions, Eur Heart J 26: 804-847
Platelet GpIIb/IIIa Inhibition: Major Intervention Trials 30 Day Death, MI, or Urgent Revascularization Trial N Odds Ratio & 95% CI Placebo IIb/IIIa EPIC 12.8% 8.3% 2099 EPILOG 11.7% 5.3% 2792 EPISTENT* 10.8% 5.3% 1603 RAPPORT 11.2% 5.8% 489 CAPTURE 15.4% 11.3% 1252 IMPACT II 11.4% 9.5% 4010 ESPRIT 10.5% 6.8% 2064 RESTORE 10.5% 8.0% 2139 0 1 2 *Stent arms only IIb/IIIa Better Placebo Better
Zusammenfassung • Akut 600mg Clopidogrel, elektiv 300mg als „loading-dose“. • ASS und Clopidogrel immer kombiniert. • Heparin 70 U/kg i. v., max. 5000 U • GP IIb/IIIa Antagonisten nicht als Standardmedikament • Bei IAP/NSTEMI GP IIb/IIIa bei Risikopatienten und geplanter PCI • Bei STEMI beste Daten für Abciximab und Stenting