Download
1 / 29
330 likes | 743 Views
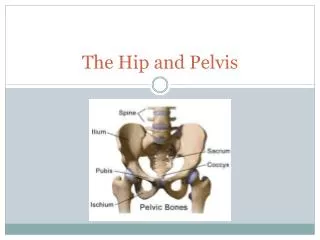
Trauma to Pelvis, Hip, Femur. Tintinalli Chapter 273. Anatomy. Iliopectineal Line. Sacrotuberous Ligament. Greater Sciatic Foramen. Sacrospinous Ligament. Lesser Sciatic Foramen. Sacrospinous Ligament. Sacrotuberous Ligament. Pelvic Trauma.

E N D
Trauma to Pelvis, Hip, Femur Tintinalli Chapter 273
Iliopectineal Line Sacrotuberous Ligament Greater Sciatic Foramen Sacrospinous Ligament Lesser Sciatic Foramen Sacrospinous Ligament Sacrotuberous Ligament
Pelvic Trauma • Secondary to MVA, pedestrian v. auto, falls in elderly, industrial accidents • Extremely vascular; therefore, pelvic fx’s must be considered in all trauma due to hypovolemia • Risk of neural, GU, GI, reproductive organ injury
History • Mechanism of injury • Determine areas of pain • Last urination or defecation • Present bladder sensation • Last food/fluid intake • Last menses/pregnancy
Physical Exam • Perineal and pelvic edema, ecchymoses, lacerations, and deformities. • Signs of pelvic fx’s • Earle’s sign -large hematoma or tenderness along fracture line or palpation of a bony prominence on rectal exam • Destot’s sign -superficial hematoma above the inguinal ligament or on the scrotum. • Roux’s sign -distance from the greater trochanter to the pubic spine is greater on one side than the other.
Physical Exam • Compress the pelvis lateral to medial, anterior to post., and through the greater trochanter. • Rectal exam- look for displacement of the prostate, rectal tone/injuries, and blood at the urethral meatus. • If a pelvic fracture is found, consider intraabdominal, retroperitoneal, gynecologic (check for vaginal injury), and urologic injuries. • High rate of fetal death is assoc. with pelvic trauma in pregnant pt. Immediate C-section must be considered.
Radiologic Evaluation • AP view pelvis mandatory in unconscious patients with multiple injuries • If needed, lateral view, AP hemipelvis, internal/external oblique hemipelvis, inlet/outlet views • CT may be needed (acetabular, sacral fx) • Angiography to determine source of bleeding
Young classification of pelvis fractures • AP compression (open book) • Type I- Disruption of the pubic symphysis <2.5cm of the diastasis; no significant post. pelvic injury. • Type II-Disruption of the pubic symphysis >2.5cm with tearing of the ant. Sacroiliac, sacrospinous and sacrotuberous ligaments. • Type III- Complete disruption of the pubic symphysis and post. Ligament complexes with hemipelvic displacement.
Young Classification • Lateral Compression • Type I- Post. Compression of the sacroiliac joint without ligament disruption; oblique pubic ramus fracture • Type II- Rupture of the post. sacroiliac ligament; pivotal int. rotation of the hemipelvis on the ant. SI joint with a crush injury of the sacrum and an oblique pubic ramus fracture. • Type III- Type II + AP compression to the contralateral hemipelvis
Young Classification • Vertical Shear • Fx of pubic rami anteriorly, while fx of sacrum, SI joint, or iliac wing are seen posteriorly. • Fractures are vertical with vertical displacement of fragments • Ligamentous injury to ant/post sacroiliac, sacrospinous, sacrotuberous and possibly symphysis
Complications of Pelvic Fx • Hemorrhage • Crystalloid, colloid, blood replacement (ave 6 units required) • Bedsheet: pelvic support & stabilization • Early ortho consultation (external fixator) • If available transarterial embolization may be needed (only 2%) only after initial treatment of fluid and blood replacement
Acetabular Fractures • Jedet-Letournel Classification • Posterior wall: post acetabular fx with post hip dislocation • Posterior Column: fx sciatic notch wt bearing portion of acetabulum obturator foramen (40% sciatic n. injury) • Anterior wall: AIIS superior ramus • Anterior column: pubic ramus iliac crest • Transverse: ant to post through acetabulum
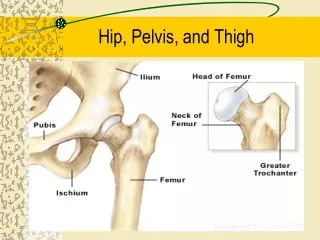
Trauma to Hip and Femur • Anatomy
Clinical Evaluation PE: deformities, shortening, rotation, lacs, bruises, compress greater trochs, ROM Radio: AP and lateral of pelvis, AP hemipelvis, Judet views Significant hip pain with wt bearing and normal xray suggest occult fx
Hip Fx Classification • Intracapsular (femoral head and neck) • Capital • Subcapital • Transcervical • Basicervical • Extracapsular • Intertrochanteric • Subtrochanteric
Femoral Head Fx • Rare: assoc. with dislocations of the hip • 10-16% posterior hip dislocations • 22-77% anterior hip dislocations • Consult ortho-reduce dislocation and attain anatomic reduction of the fracture fragment
Femoral neck fractures Subcapital, transcervical, basicervical • Displaced vs. nondisplaced • Elderly, osteoporois, women, falls/torsion • Extremity: external rotation, abduction, shortened • Pain in groin/inner thigh • Admit, ortho consult in ED
Trochanteric Fx • Greater trochanteric fractures-caused by avulsions at the insertion of the gluteus medius • Treatment conservative-surgical fixation for displacement of >1cm • Lesser trochanteric fractures-caused by avulsion secondary to forceful contraction of the iliopsoas-seen in children and young athletic adults • Pain with flexion and internal rotation-2 cm displacement needs surgical treatment
Extracapsular Fx • Intertrochanteric fractures • Women, falls, osteoporosis • Pain, swelling, ecchymosis, externally rotated and shortened • Ortho consult/admit/buck traction • Subtrochanteric fractures • Falls or major trauma • Pain, deformity, swelling, crepitance • Hemorrhage into thigh hypovolemia • Ortho consult/traction/ORIF
Anterior Hip dislocations • Femoral head rests anterior to coronal plane of acetabulum • Superior • Inferior • True ortho emergency: early closed reduction under sedation • In-line traction with flexion and internal rotation then hip abduction once the head clears the rim of acetabulum
Posterior Dislocations • Majority (80-90%) of hip dislocations • Flexed knee vs dashboard, pushing femoral head through the post. capsule • Shortened, adducted, internally rotated and flexed on PE • Associated findings • Acetabular,femoral fractures • Knee injuries • Sciatic nerve injury • Closed reduction: in line traction, flexion to 90 degrees, internal to external rotation
Femoral shaft fractures • Men, falls, industrial accidents, MVA, GSW • shortening and deformity, traction splint in pre hospital setting except in open fractures • Open fx: broad spectrum atb, debridement, copius irrigation in OR • Definitive mgmt: traction, external fixation, pins and plaster or internal fixation