Download

1 / 25
250 likes | 394 Views
Introduction to Health Insurance Exchanges. Mim Dixon USET Training Tunica Biloxi Tribe, LA May 22, 2012. The Patient Protection and Affordable Care Act (P.L. 111-148) was enacted March 23, 2010. Affordable Care Act (ACA). Insurance Reforms No lifetime limits, annual limits

E N D
Introduction toHealth Insurance Exchanges Mim Dixon USETTraining Tunica Biloxi Tribe, LA May 22, 2012
The Patient Protection and Affordable Care Act (P.L. 111-148) was enactedMarch 23, 2010.
Affordable Care Act (ACA) • Insurance Reforms • No lifetime limits, annual limits • Pre-existing conditions • Medicaid Expansion • Health Insurance Exchanges • Individuals • Small businesses • Medicare Part D “donut hole” changes • Quality, Prevention, Innovation • Health Care Workforce • Indian Health Care Improvement Act • Title X, Subtitle B, Part III, Sec. 10221
ACA Strategies to Reduce Number of Uninsured in America • Remove barriers • Insurance reform • Medicaid expansion • Create market structure (Exchanges) • Risk reduction for insurance companies • Carrots • Federal premium assistance for individuals • Federal tax credits for businesses <25 employees • Sticks • Tax penalty for uninsured • “Individual mandate” - AI/AN are exempt • Business with >50 employee • Fined $2,000/person over 30 people
What is Health Insurance Exchange? • Consumers and businesses can compare insurance plans and purchase • Federal subsidies of premiums • Enrollment in Medicaid, CHIP, Basic Health Plan (if available) • Web based approach • State or federal exchanges • Operational by January 1, 2014
“Metallic” Plans in Exchange • All plans: same Essential Health Benefits • Plans may differ: • Networks of providers • Cost of premiums, co-pays and deductibles • Actuarial values of plans equal within metallic categories • Bronze – 60% actuarial value • Silver – 70% actuarial value • Gold – 80% actuarial value • Platinum – 90% actuarial value
Exchange Functions • Select Qualified Health Plans (QHP) • Enrollment • Determine individual eligibility • Enroll people in QHPs • Contract with Navigators • Call centers • Financial management • Premiums • Tax Credits • Cost Sharing • Risk adjustments
Why are Exchanges Important for Indian Health? • New source of funding • Covers adults < 65 • Premium assistance • Up to 400% FPL • I/T/U can bill plan • Shift CHS costs to plans • Medicaid Expansion • Up to 133% FPL • Assets not counted • Covers all adults • Enroll through Exchanges
AI/AN have special protections and provisionsin ACA related to Exchanges.
American Indians and Alaska Natives are • Exempt from penalty for being uninsured • Exempt from most cost sharing in Exchange Plans • Cost sharing = deductible + co-pay • Federal government pays cost sharing to Plans • Able to enroll monthly
Exemptions from Cost Sharingfor AI/AN Enrolled in Exchange Plans • No deductibles ever • No cost sharing ever for people served in I/T/U • I/T/U collects 100% of charges from plan • No cost sharing in private sector for AI/AN with referral from I/T/U • CHS does not pay any portion of care covered by plan • For AI/AN below 300% FPL, no cost sharing in private sector without referral from I/T/U.
Premium Subsidies • AI/AN have same premium subsidies as everyone else in Exchanges • Based on Modified Adjusted Gross Income (MAGI) • Sliding scale up to 400% FPL (96%-35%) • Silver level is benchmark • Advanced tax credits • Paid to insurance company • Reconciliation at end of year
Annual Federal Subsidy of Health Insurance Premiums by Income Level for Individuals
Example: Tribe Pays Portion of Premium • Tribe pays 2% of premium for individual below 150% FPL with high cost medical needs. • Tribal Sponsorship is $690 per year. • Tribe collects payments from plan for all visits and medications provided to individual. • No cost to CHS for specialty medical care and hospital services. • More money is available to provide more services for all Tribal members.
With no cost sharing, AI/AN can choose QHPs with lower premiums.
Barriers to AI/AN Enrollment • Premium • Tribal sponsorship can eliminate barrier • Basic Health Plan can eliminate barrier • IRS rules and regulations • Advanced tax credits + reconciliation • No enrollment for non-filers • Complex rules • Basic Health Plan can eliminate barrier • Lack of insurance experience, knowledge • No motivation to enroll • Federal and State Exchange regulations
Exchange Federal Regulations • Regulations issued by two agencies • CMS, Center for Consumer Information and Insurance Oversight (CCIIO) • Department of Treasury, IRS • Federal government is deferring to States to give them flexibility. • National Tribal Participation • NIHB, MMPC, TTAG, NCAI, TSGAC
Federal Regulations Issued • Establishment of Exchanges and QHPs • Standards Related to Reinsurance, Risk Corridors and Risk Adjustment • Health Insurance Premium Tax Credit • Exchange Functions: Eligibility Determinations, Employer Standards • Medicaid Eligibility Changes under the ACA • Essential Health Benefits • Actuarial Values
More NPRMs are coming. . . • Federal payment of cost sharing for AI/AN • Tax penalties for individuals, businesses • Basic Health Program • Standards for Oversight of Quality and Reporting
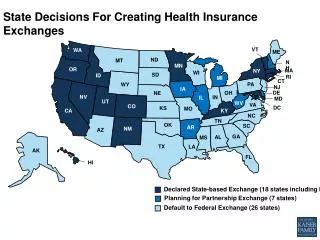
Planning at State Level • Laws, Executive Orders to Establish Exchanges • Federal Exchange Establishment Grants • Health Insurance Commissioners • Medicaid, CHIP, Basic Health Plans • Tribal Consultation • Letter from HHS Secretary to State Governors
Planning within your Tribe • Designate individual or team to become informed about ACA and Exchanges • Advocacy at State and Federal levels • Participate in Exchange planning for State • Tribal planning and budgeting • Premium payments • Provider contracts • Outreach and enrollment assistance • Communications plan
Key Dates January 1, 2013 – HHS decides whether state is ready to operate an Exchange October 15, 2013- First open enrollment period starts for Exchanges January 1, 2014 – QHPs start offering services through the Exchange
Tribal Leaders and I/T/U managementmust devote attention toHealth Exchange decisionsnow through 2013.