Download
1 / 29
290 likes | 455 Views
Incident Investigations – Key Concepts. Case Study Tower Crane Collapse. Incident Summary, Root Cause Analysis, Lessons Learnt & Corrective Actions. Incident Photo Storyboard What happened. Standard mast section. Location where workers were fatally struck - they were within 5 m of each other.

E N D
Incident Investigations – Key Concepts Case StudyTower Crane Collapse Incident Summary,Root Cause Analysis, Lessons Learnt & Corrective Actions
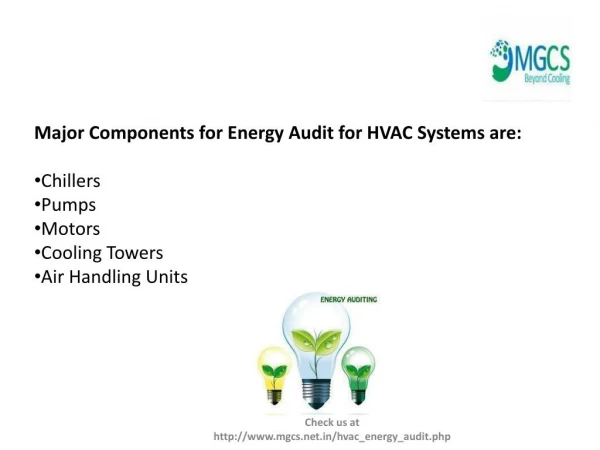
Incident Photo StoryboardWhat happened Standard mast section Location where workers were fatally struck - they were within 5 m of each other Jib Waterproofing blanket
Incident Photo Storyboard (cont’d) Crane top A-frame Operator’s cab Jib Standard mast section Climbing frame Balancing arm
Cleat on swivel section that connects with climber using 40mm dia pin Connecting Pins Eight high tensile Bolts connect mast to swivel section. Bolts were removed to swivel section
Nature of Incident: Two workers received fatal injuries when hit by falling jib of crane • WHO? • Male, Married, 3 Children, Age : 57Female, Divorced, 0 Children, Age : 30 • General labourer General labourer • Years of service: ~ 1 month Years of Service: ~ 2.5 years • Time in current position: 20 days Time in current position: 11 days • Both deceased are employees of General Contractor
WHO? - Contractual Relationships Client Project Manager Construction GC Tower Crane Supplier Crane Installation Company (Install, Maintain, Operate, Dismantle Tower Cranes #1,2,3,4) Erection Crew
What HappenedGeneral Description of Incident – Preceding Events • Nov. • the Construction Manager, visits tower crane supplier to select the cranes to be used at site. • 4 tower cranes were specified (QTZ80 x 3; QTZ40 x 1) in the supply Contract between GC and tower crane supplier. • The tower crane supplier appointed the crane installation company for installation, operation, maintenance and dismantling of the 4 cranes. • Early Dec. • The Crane Installation crew (same crew that would install Tower crane #2) attended site induction training as well as tower crane training and reviewed the safe work method statement (SWMS) before installation of Tower Crane #3. • The first crane (Tower crane #3, a QTZ80) is installed and passes inspection by National Inspection Center. • The other cranes were not installed because the site was not yet ready. One of the cranes (QTZ80A) selected was leased to another client by tower crane supplier. • Mid Dec. (up to 17) • Tower crane #1 (QTZ80) & #4 (QTZ40) were installed by crew and passed by the government inspection agency. • Tower crane #2 (QTZ63A or TC5510), (manufactured in December), was delivered to the site with some components missing. Crane delivery was rejected.
What HappenedGeneral Description of Incident – Preceding Events • Dec. 19 • Missing components for crane #2 arrive - GC accept the crane, (which was not the one ordered + copy of manufacturer’s test result report was for the ordered crane, not the one actually received by the GC). • The manufacturer’s manual for TC5510 (the actual crane on site) was provided with the crane. • GC apply for a Work Permit to use a mobile crane to install tower crane #2. PM approve permit. • Dec. 20 • The erection crew start to install tower crane #2 on site (same crew that installed the other 3 cranes on site). An exclusion zone around the installation area is created. • The crane was erected to about 9 meters high (3 of the 10 standard mast sections) other 7 sections placed on the ground 25 meters from base of the tower crane #2. • The installation was stopped by PM because it was getting dark. Pending tasks included: jib installation; (2) Climbing frame connection to the swivel (note: the 4 pins used to secure the climbing frame to the swivel were not put in place); (3) filling hydraulic oil tank for climbing frame (2 drums of oil (90 liters) placed about 20 meters from the base of the tower crane #2). • The crew and GC planned to install the jib in the early morning of December 22, 2006 as the government inspection had been scheduled for December 22, 2006.
What HappenedGeneral Description of Incident – Preceding Events • Dec. 21 • The installation of tower crane #2 continued without application for a new Permit (even though the mobile crane was still required). • The jib was installed in the morning with the two other pending tasks still incomplete. • Tower crane #2 was inspected by National Inspection Center (SCMIC). • Dec. 22 • PM safety leader states that a Permit to Work is needed daily for use tower cranes - same form for approval of mobile crane use. This new requirement was communicated between PM safety team and the GC safety team verbally. • Dec. 23 • Pass Certificate and inspection report, issued by authorities – with 2 action items: (1) the earthing for the crane was exposed; (2) the power panel for the crane was not separated from the crane. Report noted that the climbing frame was not connected to the swivel. • The report also stated that the bolts connecting the installed 3 standard mast sections were tightened to specification, but it was found during the investigation that these bolts were only hand-tight. • The crew leader only half filled the climbing frame hydraulic oil tank as he ran out of oil.
What HappenedGeneral Description of Incident – Preceding Events • Dec. 24 7:00 a.m. • The crew leader used tower crane #2 –to lift and move 5 rolls of water-proofing material without a permit to use the tower crane. 8:00 a.m. • GC safety engineer initiated an application for a work permit for lifting of water-proofing material (not crane climbing) using tower crane #2. 9:00 a.m. – 9:30 a.m. • The form was returned back to GC without any rejection or approval comments on the form. Verbal rejection was based on the earthing issues previously identified. • GC submits a copy of the Pass Certificate and Authority Inspection Report to PM. • Crane Erection crew leave site due to lack of work and return to dormitory Throughout the day, brickwork was being performed on the footings of the basement slab.
What HappenedGeneral Description of Incident – Preceding EventsDec. 24 (continued) 12:00 p.m. • The tower crane installation ltd supervisor/manager delivers 2 additional walkie-talkies to site then visits the crane crew during lunch at their dormitory and tells the crew leader to jack up tower crane #2 to a height of 17 meters (3 more standard mast sections). 12:30 p.m. • The crew leader starts to prepare tower crane #2 for the jacking operation - attempts to move the climbing frame up to connect the frame to the swivel, but fails because there was an inadequate amount of hydraulic oil in the tank of the climbing frame. He then lifted and moved 4 of the 7 standard mast sections on the ground closer to the base of the crane and kept one standard mast section lifted hanging in the air when he left the cab. 1:00 p.m. • The crew leader and flagman hand-lifted one drum of hydraulic oil to the work platform which was attached to the climbing frame, and started to fill the hydraulic oil tank. 1:30 p.m. • The crew leader instructs the crane operator to loosen the 8 bolts securing the top mast section to the slewing ring support. The crew leader then finds that the hydraulic oil tank was still under pressured to climb. The crew leader and operator #2 went over to tower crane #4 and extracted about one drum of hydraulic oil from the tank of crane #4
What HappenedGeneral Description of Incident – Preceding Events Dec. 24 (continued) 2:00 p.m. • Operator #1 loosens and removes the 8 bolts connecting the swivel and the mast, leaving one mast section hanging in the air to keep balance. • PM’s entire site team started an accident investigation training class in site trailer. • Hydraulic oil tank of climbing frame of crane #2 filled – climbing frame operational. 3:00 p.m • The crew leader instructs tower crane Operator #1 to climb up to the operator’s cab to move the hanging standard mast section onto the working platform. • Operator #1 pulled the hanging standard mast section towards the climbing frame platform. The jib of the crane tilted upwards and the counter-jib tilted downwards. The jib and crane top sections lost their balance and toppled from the mast.. • Workers in the excavation area including the flagman (Op. #2) panicked and started to run in different directions to avoid being hit. Female worker was struck on her head and male worker was struck on his body by the tie-line of the jib. • Operator #1 stayed in cab by holding onto the window frame - received minor injuries to his forearm.
What HappenedGeneral Description of Incident – Incident EventsDec. 24 (continued) 3:12 p.m. • Workers & site engineers heard the collapse and responded to the scene of the injured. Some went to the site’s First Aid station. • Some engineers/workers phoned for an ambulance from the Public First Aid Center. 3:15 p.m. • The site First Aid responder arrived at the scene of the injured. PM and GC project teams were alerted and went to the scene. 3:20 p.m. • The first ambulance arrived. Wang BH was carried onto the ambulance by the workers. He was still conscious. A call for a second ambulance was made. 4:00 p.m. • Female worker was pronounced dead. 5:55 p.m. • Male worker was pronounced dead during surgery.
What HappenedRelevant Issues: • Both GC and PM were NOT informed of the climbing task before hand. • The Safe Work Method Statements (SWMS) for crane installation, operation, maintenance and dismantling does not specify the process of jacking up a crane • The SWMS was not updated for installation of tower cranes #4, #1 or #2, nor was it communicated to the crew before the installation of #4, #1 and #2. • No procedure specifically requires a work permit for crane jacking, although there is a general requirement in the Task Hazard Analysis process. • The crew leader is certified for crane operating, signaling, installation and dismantling. The 2 operators and 1 flagman are certified for crane operating and signaling only, not installation or dismantling. • Operator #1 who is the nephew and trainee of the crew leader, is about 20 years old with about 1.5 years experience of crane operation (amount of operating hours unknown). This was his first time to operating crane type TC5510. • It was also found that he had been on duty for 15 hours operating tower crane #3 on Dec. 25, 2006, one day before the incident. (rest time unknown)
What Happened -Relevant Issues • Before removing the swivel bolts, Operator #1 states that he saw the 4 connection pins of the climbing section lying on the platform, but did not verbalize this to the crew leader. • During interviews, the crew leader having seen the pins states that he did not remember that swivel had not been connected to the climbing frame. • Operator #1 stated that he understood the direction from the crew leader for “loosen” as “loosen and remove” the bolts. • Crew Supervisor did not remember that the swivel was NOT connected to the climbing frame (4 pins not placed in), and the 8 bolts connecting the swivel to the installed mast were all removed. No checks were made on this safety critical issue. • No exclusion zone around the crane is created, however, flagman states that he attempted to direct 4 workers who were doing soil backfilling to leave the area. Two of them left and the other 2 refused to go. (Unable to verify if the request was made and if the workers that remained in the area were those fatally injured.)
Root Cause Analysis Exercise In Small Groups (each table)….. • Analyse the evidence in the case study • Identify the critical factors and their immediate causes • Using the ‘5 whys’ approach identify the causes of each critical factor • Identify the term from the underlying factors terminology which best describes the key underlying cause(s) of each critical factor (if time allows - produce a summary diagram of the key underlying factors from the ‘5 whys’ analysis identifying the root causes). • Identify the key corrective actions and Lessons Learnt
Incident Summary • Four tower cranes mobilized on a construction project site • Tower crane #2 (last crane to mobilize) collapses • Crane climbing operation commenced without following proper procedures • PM site project operations team unaware of work activity • No exclusion zone established during jacking operation - workers associated with basement construction activities are working near tower crane #2 • Crane manufacturers’ erection procedures not followed • Unsecured tower crane jib becomes unbalanced and topples over • Two workers involved in basement construction are fatally injured when struck by the falling crane jib
Root Causes Analysis – Summary of Critical Factors & Underlying Causes for Crane Jib Collapse Incident Critical Factors Crew Leader Instructs Driver To Remove Head Bolts Crew Leader Forgot Pins Missing Operation not observed PM staff in training - GF on leave PM Permit system lacks clarity - only for crane operation but not for erection/jacking JF1 Work conducted without PM permit or notification to GC & no exclusion zone Inexperienced Driver Saw Pins Missing- but said nothing No Checking Procedure before removing bolts etc Communication and Change Management Org F6 and F8 Poor SWMS - did not deal with climbing process Crane operation subcontractor – no formal H&S system Competence PF1 Crew Supervision JF3 Contractor Management Org F1 GC did not conduct H&S pre-qual nor follow H&S reqs GC Did Not Pick Up Issue Perception of Risk PF8 Culture: Face - Crew Leader = Uncle PM Review Did Not Pick Up Issue PM Safety Management System Org F7 PM did not check that GC did the pre-qual nor approve GCs sub Resources to implement safety standards Org F11 Inadequate THA RA SWMS, Task Planning, process JF1 JF2
Immediate and Root Causes Immediate Causes Root Causes Factors Identified • Securing pins to attach climbing frame to slewing ring support not installed Low level of crane operator competence Personal Factors Poor supervision of crane crew activities • High tensile bolts removed from slewing ring Non-compliance with aspects of Safety Management System Job / Process/ Procedure Factors RA, SWMS, THA, permit process was not adequately implemented Lack process for control of crane erection, climbing & dismantling • Mast section trolleyed in moving jib out of balance causing crane to topple over Poor Contractor Management PM Resources Organizational Factors Lack of Communication & Work supervision • No exclusion zone established allowing workers to be hit by falling jib
Corrective Action Corrective and preventative action plans developed to address: • Project re-start • Root cause and other causes of the accident • EHS program implementation follow-up
Preventative Action 1) Operator Competence • FINDING: Inadequate experience and level of training of crane operators. Cannot assume that crane operators with a license certified by the government are competent. • ACTIONS: • Introduce screening of operator’s experience during induction • Introduce crane operator testing • Introduce minimum experience requirements for personnel involved in high risk tasks (5 yrs for crane operators) 2) Supervision • FINDING: Inadequate supervision of crane crew operations • ACTIONS: • Replace crane crew subcontractor • Test competence of supervisor • Brief supervisor on PM requirements inc weekly safety meetings and following PtW • Implement supervisor skills workshop for GC and Subcontractor Supervisors and additional safety induction for crew leaders
Preventative Action 3) Non-Compliance with risk safety management system • FINDING: Risk Assessment, Safe Work Method Statement, Task Hazard Analysis and Permit to Work procedures were not completely implemented • ACTIONS: • PM to review risk assessment for missing high risk operations • Implement a look-ahead process for HROs - update project risk assessment monthly • Implement a process in addition to SWMS for all high risk operations • Add rigor in identifying risks, preparing and reviewing of SWMS - critically review all current SWMS for level of detail and robustness • PM to conduct regional peer review of current and future SWMS prior to approval • PM to employ a crane specialist (other high risk specialists as needed) • New permit process specific for crane erection, climbing, & dimsantling • Train PM, GC, and Subcontractors on high risk operation requirements, and permit-to-work process and requirements
Preventative Action 4) Poor Contractor Management Subcontractor Pre-qualification – Process established but not followed • FINDINGS: GC did not use their described process and PM did not do verification checks • ACTIONS: • PM to maintain master list of all approved contractors cleared to enter the site • PM to prepare list of subs that will perform high risk work activities • PM to pre-qualify sub-tier contractors for all contractors involved in high risk operations • PM to verify Contractor pre-qualification by GC • PM to spot-check subcontractor pre-qualifications for non-high-risk contractors • PM to review recommendations of Subcontractors • Retrain entire PM team in project pre-qualification requirements
Preventative Action 4) Lack of Contractor Management cont. FINDING: Contractor & Subcontractor Oversight needs enhancement • ACTIONS: • Restructure PM & GC Project Teams • All PM staff & contractor supervisors are to be re-inducted about revised procedures • Crew and supervisor sign-off on Safe Work Method Statements (SWMS) and Task Hazard Analysis (THA) • Improve PM auditing & review of site safety management systems • PM to always have site personnel in the field overseeing contractors working • PM to create minimum EHS standards for all Subcontractor safety personnel • All project safety personnel reviewed and approved by PM onsite safety leader and PM regional safety manager 5) Resources • FINDING: Resources inadequate to ensure contractor control and full operation of SMS • ACTIONS: • Ensure that proposed and accepted resources are in place • Add EHS Program Manager & change Site Safety Manager • Ensure back-up resources are in place for team member vacations
Preventative Action 6) Communication & Change Management • FINDING: There is a lack of communication between PM and Contractors • ACTIONS: PM to be involved in GC-Subcontractor interface • Hold daily schedule coordination meetings (PM, GC, & Subs) – include EHS • Worker safety briefing at the commencement of each shift • Weekly safety meetings for PM • Weekly safety meeting with PM, GC & subs in attendance • Weekly Coordination team meeting (PM, GC, Subs) • Conduct a look ahead of high risk operations and communicate the information among site team – monthly (PM, GC, Subs) • Establish work permit board at the site office to note all work permits issued (Permits issued to whom, for what operations and the location of the work) • Establish monthly Safety Leadership Team calls (Senior leadership GE, PM, GC & Subs)
Lessons Learnt – PM Global EHS Actions • Issued Global Crane Safety Alert to introduce new policy and procedures, including permit system for controlling crane erection, climbing & dismantling operations; • Use incident investigation analysis as a case study in H&S management systems and root cause analysis training workshops. Three planned in next two months to train around 50 staff. • Improve process of contactor pre-qualification, selection and management (including communications and change management). • Consider more carefully resource issues and client demands before taking on projects
Accident Investigation– Key Concepts Review of issues covered • Accident - Meanings & Paradigms • Accident causation theories • What is an investigation and why do it? • Interviewing witnesses • Analytical Methods • Case study


![Report on Global Tower Crane Market [2015-2019]](https://cdn4.slideserve.com/7280573/slide1-dt.jpg)